Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Visceral leishmaniasis
Visceral leishmaniasis (VL), also known as kala-azar (Hindi: kālā āzār, "black sickness") or "black fever", is the most severe form of leishmaniasis and, without proper diagnosis and treatment, is associated with high fatality. Leishmaniasis is a disease caused by protozoan parasites of the genus Leishmania.
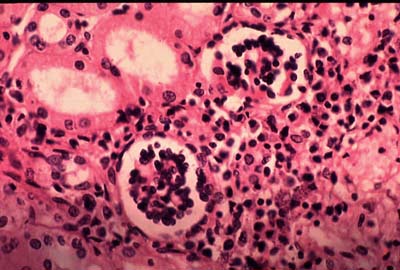
The parasite migrates to the internal organs such as the liver, spleen (hence "visceral"), and bone marrow, and, if left untreated, will almost always result in the death of the host. Signs and symptoms include fever, weight loss, fatigue, anemia, and substantial swelling of the liver and spleen. Of particular concern, according to the World Health Organization (WHO), is the emerging problem of HIV/VL co-infection.
VL is the second-largest parasitic killer in the world (after malaria), responsible for an estimated 20,000 to 30,000 deaths each year worldwide.
Upendranath Brahmachari synthesised urea stibamine (carbostibamide) in 1922 and determined that it was an effective substitute for the other antimony-containing compounds in the treatment of VL caused by Leishmania donovani.
When people develop visceral leishmaniasis, the most typical symptoms are fever and the enlargement of the spleen, with enlargement of the liver sometimes being seen as well. The blackening of the skin that gave the disease its common name in India does not appear in most strains of the disease. The other symptoms are easily mistaken for those of malaria. Misdiagnosis is dangerous, as without proper treatment, the mortality rate for kala-azar is close to 100%. L. donovani itself is not usually the direct cause of death in people with kala-azar, however. Pneumonia, tuberculosis, and dysentery are omnipresent in the immuno-depressed regions where leishmaniasis thrives, and, as with AIDS, it is these opportunistic infections that are more likely to kill, flaring up in a host whose immune system has been weakened by the L. donovani infection. Progress of the disease is extremely variable, taking anywhere from one to twenty weeks, but a typical duration for the Sudanese strain of the disease is narrower, between twelve and sixteen weeks.
Even with recovery, kala-azar does not always leave its hosts unmarked. Some time after successful treatment—generally a few months with African kala-azar, or as much as several years with the Indian strain—a secondary form of the disease may set in, called post kala-azar dermal leishmaniasis, or PKDL. This condition manifests first as small, measles-like skin lesions on the face, which gradually increase in size and spread over the body. Eventually, the lesions may coalesce to form disfiguring, swollen structures resembling leprosy, and occasionally cause blindness if they spread to the eyes. (This disease is not the same as cutaneous leishmaniasis, a milder disease caused by another protozoan of the Leishmania genus, which also causes skin lesions.)
Two species of Leishmania are known to give rise to the visceral form of the disease. The species commonly found in East Africa and the Indian subcontinent is L. donovani and the species found in Europe, North Africa, and Latin America is L. infantum, also known as L. chagasi.
The insect vectors are species of sandfly of the genus Phlebotomus in the Old World, and of Lutzomyia in the New World. Sandflies are tiny flies, measuring 3–6 mm long by 1.5–3 mm in diameter, and are found in tropical or temperate regions throughout the world. The sandfly species Lutzomyia longipalpis is the primary vector of this disease. The larvae grow in warm, moist organic matter around human habitations (such as old trees, house walls, or waste), making them hard to eradicate.
Hub AI
Visceral leishmaniasis AI simulator
(@Visceral leishmaniasis_simulator)
Visceral leishmaniasis
Visceral leishmaniasis (VL), also known as kala-azar (Hindi: kālā āzār, "black sickness") or "black fever", is the most severe form of leishmaniasis and, without proper diagnosis and treatment, is associated with high fatality. Leishmaniasis is a disease caused by protozoan parasites of the genus Leishmania.
The parasite migrates to the internal organs such as the liver, spleen (hence "visceral"), and bone marrow, and, if left untreated, will almost always result in the death of the host. Signs and symptoms include fever, weight loss, fatigue, anemia, and substantial swelling of the liver and spleen. Of particular concern, according to the World Health Organization (WHO), is the emerging problem of HIV/VL co-infection.
VL is the second-largest parasitic killer in the world (after malaria), responsible for an estimated 20,000 to 30,000 deaths each year worldwide.
Upendranath Brahmachari synthesised urea stibamine (carbostibamide) in 1922 and determined that it was an effective substitute for the other antimony-containing compounds in the treatment of VL caused by Leishmania donovani.
When people develop visceral leishmaniasis, the most typical symptoms are fever and the enlargement of the spleen, with enlargement of the liver sometimes being seen as well. The blackening of the skin that gave the disease its common name in India does not appear in most strains of the disease. The other symptoms are easily mistaken for those of malaria. Misdiagnosis is dangerous, as without proper treatment, the mortality rate for kala-azar is close to 100%. L. donovani itself is not usually the direct cause of death in people with kala-azar, however. Pneumonia, tuberculosis, and dysentery are omnipresent in the immuno-depressed regions where leishmaniasis thrives, and, as with AIDS, it is these opportunistic infections that are more likely to kill, flaring up in a host whose immune system has been weakened by the L. donovani infection. Progress of the disease is extremely variable, taking anywhere from one to twenty weeks, but a typical duration for the Sudanese strain of the disease is narrower, between twelve and sixteen weeks.
Even with recovery, kala-azar does not always leave its hosts unmarked. Some time after successful treatment—generally a few months with African kala-azar, or as much as several years with the Indian strain—a secondary form of the disease may set in, called post kala-azar dermal leishmaniasis, or PKDL. This condition manifests first as small, measles-like skin lesions on the face, which gradually increase in size and spread over the body. Eventually, the lesions may coalesce to form disfiguring, swollen structures resembling leprosy, and occasionally cause blindness if they spread to the eyes. (This disease is not the same as cutaneous leishmaniasis, a milder disease caused by another protozoan of the Leishmania genus, which also causes skin lesions.)
Two species of Leishmania are known to give rise to the visceral form of the disease. The species commonly found in East Africa and the Indian subcontinent is L. donovani and the species found in Europe, North Africa, and Latin America is L. infantum, also known as L. chagasi.
The insect vectors are species of sandfly of the genus Phlebotomus in the Old World, and of Lutzomyia in the New World. Sandflies are tiny flies, measuring 3–6 mm long by 1.5–3 mm in diameter, and are found in tropical or temperate regions throughout the world. The sandfly species Lutzomyia longipalpis is the primary vector of this disease. The larvae grow in warm, moist organic matter around human habitations (such as old trees, house walls, or waste), making them hard to eradicate.