Recent from talks
DNA vaccine
Knowledge base stats:
Talk channels stats:
Members stats:
DNA vaccine
A DNA vaccine is a type of vaccine that transfects a specific antigen-coding DNA sequence into the cells of an organism as a mechanism to induce an immune response.
DNA vaccines work by injecting genetically engineered plasmid containing the DNA sequence encoding the antigen(s) against which an immune response is sought, so the cells directly produce the antigen, thus causing a protective immunological response. DNA vaccines have theoretical advantages over conventional vaccines, including the "ability to induce a wider range of types of immune response". Several DNA vaccines have been tested for veterinary use. In some cases, protection from disease in animals has been obtained, in others not. Research is ongoing over the approach for viral, bacterial and parasitic diseases in humans, as well as for cancers. In August 2021, Indian authorities gave emergency approval to ZyCoV-D. Developed by Cadila Healthcare, it is the first DNA vaccine approved for humans.
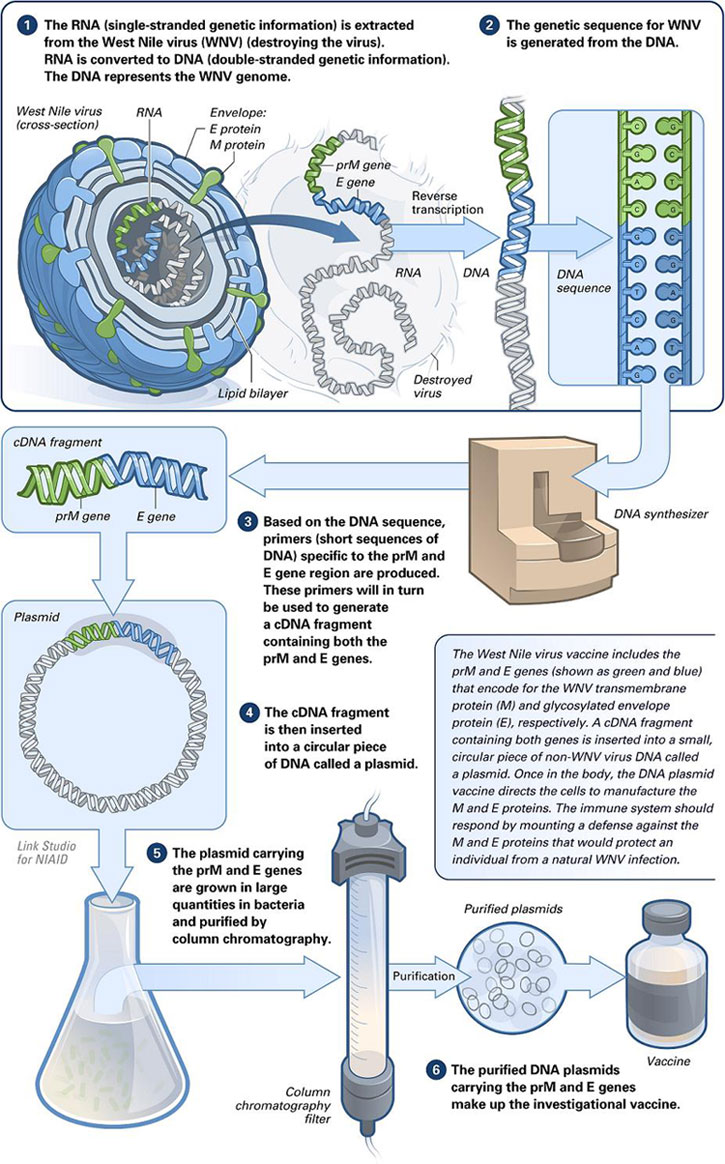
Conventional vaccines contain either specific antigens from a pathogen, or attenuated viruses which stimulate an immune response in the vaccinated organism. DNA vaccines are members of the genetic vaccines, because they contain a genetic information (DNA or RNA) that codes for the cellular production (protein biosynthesis) of an antigen. DNA vaccines contain DNA that codes for specific antigens from a pathogen. The DNA is injected into the body and taken up by cells, whose normal metabolic processes synthesize proteins based on the genetic code in the plasmid that they have taken up. Because these proteins contain regions of amino acid sequences that are characteristic of bacteria or viruses, they are recognized as foreign and when they are processed by the host cells and displayed on their surface, the immune system is alerted, which then triggers immune responses. Alternatively, the DNA may be encapsulated in protein to facilitate cell entry. If this capsid protein is included in the DNA, the resulting vaccine can combine the potency of a live vaccine without reversion risks.[citation needed]
In 1983, Enzo Paoletti and Dennis Panicali at the New York Department of Health devised a strategy to produce recombinant DNA vaccines by using genetic engineering to transform ordinary smallpox vaccine into vaccines that may be able to prevent other diseases. They altered the DNA of cowpox virus by inserting a gene from other viruses (namely Herpes simplex virus, hepatitis B and influenza). In 1993, Jeffrey Ulmer and co-workers at Merck Research Laboratories demonstrated that direct injection of mice with plasmid DNA encoding a flu antigen protected the animals against subsequent experimental infection with influenza virus. In 2016 a DNA vaccine for the Zika virus began testing in humans at the National Institutes of Health. The study was planned to involve up to 120 subjects aged between 18 and 35. Separately, Inovio Pharmaceuticals and GeneOne Life Science began tests of a different DNA vaccine against Zika in Miami. The NIH vaccine is injected into the upper arm under high pressure. Manufacturing the vaccines in volume remained unsolved as of August 2016. Clinical trials for DNA vaccines to prevent HIV are underway.
In August 2021, Indian authorities gave emergency approval to ZyCoV-D. Developed by Cadila Healthcare, it is the first DNA vaccine against COVID-19.
As of 2021[update] no DNA vaccines have been approved for human use in the United States. Few experimental trials have evoked a response strong enough to protect against disease and the technique's usefulness remains to be proven in humans.
A veterinary DNA vaccine to protect horses from West Nile virus has been approved. Another West Nile virus vaccine has been tested successfully on American robins.
DNA immunization is also being investigated as a means of developing antivenom sera. DNA immunization can be used as a technology platform for monoclonal antibody induction.
Hub AI
DNA vaccine AI simulator
(@DNA vaccine_simulator)
DNA vaccine
A DNA vaccine is a type of vaccine that transfects a specific antigen-coding DNA sequence into the cells of an organism as a mechanism to induce an immune response.
DNA vaccines work by injecting genetically engineered plasmid containing the DNA sequence encoding the antigen(s) against which an immune response is sought, so the cells directly produce the antigen, thus causing a protective immunological response. DNA vaccines have theoretical advantages over conventional vaccines, including the "ability to induce a wider range of types of immune response". Several DNA vaccines have been tested for veterinary use. In some cases, protection from disease in animals has been obtained, in others not. Research is ongoing over the approach for viral, bacterial and parasitic diseases in humans, as well as for cancers. In August 2021, Indian authorities gave emergency approval to ZyCoV-D. Developed by Cadila Healthcare, it is the first DNA vaccine approved for humans.
Conventional vaccines contain either specific antigens from a pathogen, or attenuated viruses which stimulate an immune response in the vaccinated organism. DNA vaccines are members of the genetic vaccines, because they contain a genetic information (DNA or RNA) that codes for the cellular production (protein biosynthesis) of an antigen. DNA vaccines contain DNA that codes for specific antigens from a pathogen. The DNA is injected into the body and taken up by cells, whose normal metabolic processes synthesize proteins based on the genetic code in the plasmid that they have taken up. Because these proteins contain regions of amino acid sequences that are characteristic of bacteria or viruses, they are recognized as foreign and when they are processed by the host cells and displayed on their surface, the immune system is alerted, which then triggers immune responses. Alternatively, the DNA may be encapsulated in protein to facilitate cell entry. If this capsid protein is included in the DNA, the resulting vaccine can combine the potency of a live vaccine without reversion risks.[citation needed]
In 1983, Enzo Paoletti and Dennis Panicali at the New York Department of Health devised a strategy to produce recombinant DNA vaccines by using genetic engineering to transform ordinary smallpox vaccine into vaccines that may be able to prevent other diseases. They altered the DNA of cowpox virus by inserting a gene from other viruses (namely Herpes simplex virus, hepatitis B and influenza). In 1993, Jeffrey Ulmer and co-workers at Merck Research Laboratories demonstrated that direct injection of mice with plasmid DNA encoding a flu antigen protected the animals against subsequent experimental infection with influenza virus. In 2016 a DNA vaccine for the Zika virus began testing in humans at the National Institutes of Health. The study was planned to involve up to 120 subjects aged between 18 and 35. Separately, Inovio Pharmaceuticals and GeneOne Life Science began tests of a different DNA vaccine against Zika in Miami. The NIH vaccine is injected into the upper arm under high pressure. Manufacturing the vaccines in volume remained unsolved as of August 2016. Clinical trials for DNA vaccines to prevent HIV are underway.
In August 2021, Indian authorities gave emergency approval to ZyCoV-D. Developed by Cadila Healthcare, it is the first DNA vaccine against COVID-19.
As of 2021[update] no DNA vaccines have been approved for human use in the United States. Few experimental trials have evoked a response strong enough to protect against disease and the technique's usefulness remains to be proven in humans.
A veterinary DNA vaccine to protect horses from West Nile virus has been approved. Another West Nile virus vaccine has been tested successfully on American robins.
DNA immunization is also being investigated as a means of developing antivenom sera. DNA immunization can be used as a technology platform for monoclonal antibody induction.
Recent media