Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Human T-lymphotropic virus 1
Human T-cell lymphotropic virus type 1 or human T-lymphotropic virus (HTLV-I or HTLV-1), also called the adult T-cell lymphoma virus type 1, is a retrovirus of the human T-lymphotropic virus (HTLV) family.
Most people with HTLV-1 infection do not appear to develop health conditions that can be directly linked to the infection. However, there is a subgroup of people who experience severe complications. The most well characterized are adult T-cell lymphoma (ATL) and HTLV-I-associated myelopathy/Tropical spastic paraparesis (HAM/TSP), both of which are only diagnosed in individuals testing positive to HTLV-1 infection. The estimated lifetime risk of ATL among people with HTLV-1 infection is approximately 5%, while that of HAM/TSP is approximately 2%.
In 1977, Adult T-cell lymphoma (ATL) was first described in a case series of individuals from Japan. The symptoms of ATL were different from other lymphomas known at the time. The common birthplace shared amongst most of the ATL patients was suggestive of an infectious cause, referred to as ATLV. Strikingly, ATLV had the transforming activity in vitro. These studies established that HTLV-1 was the causitive agent of ATL. The retrovirus is now generally called HTLV-I because later studies proved that ATLV is the same as the firstly identified human retrovirus called HTLV discovered by Bernard Poiesz and Francis Ruscetti and their co-workers in the laboratory of Robert C. Gallo at the National Cancer Institute. Persistent lifelong infection is established when HTLV-1 integrates into the host genome as a provirus. A patient infected with HTLV-1 can be diagnosed when antibodies against HTLV-1 are detected in the serum.
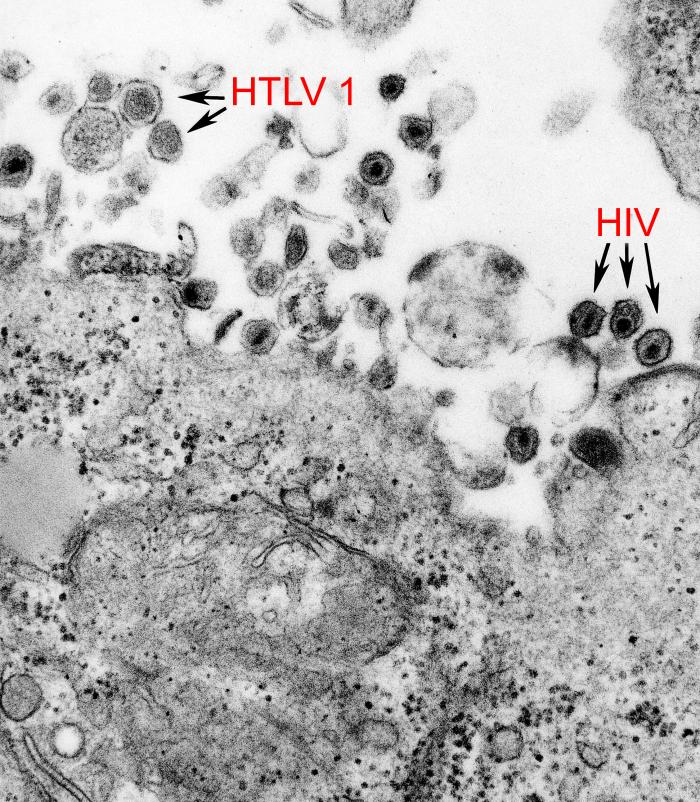
HTLV-1 is a retrovirus belonging to the family retroviridae and the genus deltaretrovirus. It has a positive-sense RNA genome that is reverse transcribed into DNA and then integrated into the cellular DNA. Once integrated, HTLV-1 continues to exist only as a provirus which can spread from cell to cell through a viral synapse. Few, if any, free virions are produced and there is usually no detectable virus in the blood plasma though the virus is present in genital secretions. Like HIV, HTLV-1 predominantly infects CD4+ T cells.
The viral RNA is packed into the icosahedral capsid inside the proteinaceous inner envelope. The lipid outer envelope is of host cell origin but contains viral transmembrane and surface proteins. The virion is spherical with a diameter of about 100 nm.
HTLV-1 is genetically classified into seven subtypes, each defined by a unique geographic distribution influenced by population migration. The most globally widespread is the cosmopolitan subtype A, which further branches into several subgroups: transcontinental, Japanese, West African, North African, Senegalese, and Afro-Peruvian. While subtypes B, D, E, F, and G are localized to distinct regions in Africa, subtype C is predominant in Australia and Oceania.
HTLV-1 is believed to have originated from the simian T-lymphotropic virus type 1 (STLV-1), a retrovirus prevalent among numerous nonhuman primates in intertropical Africa. This theory is supported by the significant genetic diversity of HTLV-1 subtypes in Africa, potentially arising from repeated zoonotic transmissions during human interactions with STLV-1 endemic nonhuman primates. This correlation is further reinforced by the observation that individuals bitten by nonhuman primates exhibit HTLV-1 strains with sequences remarkably homologous to the STLV-1 found in local primate species.
The global distribution of HTLV-I is highly heterogeneous, with focal occurrence in diverse regions. Within areas where HTLV-I is found, its occurrence varies considerably, with endemic clusters often situated near populations with lower prevalence. This pattern might be influenced by the founder effect, suggesting prolonged viral transmission within isolated groups, but this theory warrants further investigation. Consistent findings reveal that HTLV-1 prevalence increases with age and is usually higher in adult females than males. Areas broadly regarded as having endemic regions include Japan, Iran, the Americas, the Caribbean, Melanesia, Central and West Africa, and Australia. Globally, there remains a lack of robust data from populous countries like India and Nigeria and most of North and East Africa. As such, current global prevalence estimates, which are based on known endemic regions, likely underestimate the true global prevalence.
Hub AI
Human T-lymphotropic virus 1 AI simulator
(@Human T-lymphotropic virus 1_simulator)
Human T-lymphotropic virus 1
Human T-cell lymphotropic virus type 1 or human T-lymphotropic virus (HTLV-I or HTLV-1), also called the adult T-cell lymphoma virus type 1, is a retrovirus of the human T-lymphotropic virus (HTLV) family.
Most people with HTLV-1 infection do not appear to develop health conditions that can be directly linked to the infection. However, there is a subgroup of people who experience severe complications. The most well characterized are adult T-cell lymphoma (ATL) and HTLV-I-associated myelopathy/Tropical spastic paraparesis (HAM/TSP), both of which are only diagnosed in individuals testing positive to HTLV-1 infection. The estimated lifetime risk of ATL among people with HTLV-1 infection is approximately 5%, while that of HAM/TSP is approximately 2%.
In 1977, Adult T-cell lymphoma (ATL) was first described in a case series of individuals from Japan. The symptoms of ATL were different from other lymphomas known at the time. The common birthplace shared amongst most of the ATL patients was suggestive of an infectious cause, referred to as ATLV. Strikingly, ATLV had the transforming activity in vitro. These studies established that HTLV-1 was the causitive agent of ATL. The retrovirus is now generally called HTLV-I because later studies proved that ATLV is the same as the firstly identified human retrovirus called HTLV discovered by Bernard Poiesz and Francis Ruscetti and their co-workers in the laboratory of Robert C. Gallo at the National Cancer Institute. Persistent lifelong infection is established when HTLV-1 integrates into the host genome as a provirus. A patient infected with HTLV-1 can be diagnosed when antibodies against HTLV-1 are detected in the serum.
HTLV-1 is a retrovirus belonging to the family retroviridae and the genus deltaretrovirus. It has a positive-sense RNA genome that is reverse transcribed into DNA and then integrated into the cellular DNA. Once integrated, HTLV-1 continues to exist only as a provirus which can spread from cell to cell through a viral synapse. Few, if any, free virions are produced and there is usually no detectable virus in the blood plasma though the virus is present in genital secretions. Like HIV, HTLV-1 predominantly infects CD4+ T cells.
The viral RNA is packed into the icosahedral capsid inside the proteinaceous inner envelope. The lipid outer envelope is of host cell origin but contains viral transmembrane and surface proteins. The virion is spherical with a diameter of about 100 nm.
HTLV-1 is genetically classified into seven subtypes, each defined by a unique geographic distribution influenced by population migration. The most globally widespread is the cosmopolitan subtype A, which further branches into several subgroups: transcontinental, Japanese, West African, North African, Senegalese, and Afro-Peruvian. While subtypes B, D, E, F, and G are localized to distinct regions in Africa, subtype C is predominant in Australia and Oceania.
HTLV-1 is believed to have originated from the simian T-lymphotropic virus type 1 (STLV-1), a retrovirus prevalent among numerous nonhuman primates in intertropical Africa. This theory is supported by the significant genetic diversity of HTLV-1 subtypes in Africa, potentially arising from repeated zoonotic transmissions during human interactions with STLV-1 endemic nonhuman primates. This correlation is further reinforced by the observation that individuals bitten by nonhuman primates exhibit HTLV-1 strains with sequences remarkably homologous to the STLV-1 found in local primate species.
The global distribution of HTLV-I is highly heterogeneous, with focal occurrence in diverse regions. Within areas where HTLV-I is found, its occurrence varies considerably, with endemic clusters often situated near populations with lower prevalence. This pattern might be influenced by the founder effect, suggesting prolonged viral transmission within isolated groups, but this theory warrants further investigation. Consistent findings reveal that HTLV-1 prevalence increases with age and is usually higher in adult females than males. Areas broadly regarded as having endemic regions include Japan, Iran, the Americas, the Caribbean, Melanesia, Central and West Africa, and Australia. Globally, there remains a lack of robust data from populous countries like India and Nigeria and most of North and East Africa. As such, current global prevalence estimates, which are based on known endemic regions, likely underestimate the true global prevalence.