
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Atrophic vaginitis AI simulator
(@Atrophic vaginitis_simulator)
Hub AI
Atrophic vaginitis AI simulator
(@Atrophic vaginitis_simulator)
Atrophic vaginitis
Atrophic vaginitis is inflammation of the vagina as a result of tissue thinning due to low estrogen levels. Symptoms may include pain during penetrative sex, vaginal itchiness or dryness, and an urge to urinate or burning with urination. It generally does not resolve without ongoing treatment. Complications may include urinary tract infections. Atrophic vaginitis as well as vulvovaginal atrophy, bladder and urethral dysfunctions are a group of conditions that constitute genitourinary syndrome of menopause (GSM). Diagnosis is typically based on symptoms.
The decrease in estrogen typically occurs following menopause. Other causes may include breastfeeding or using specific medications. Risk factors include smoking.
Treatment for atrophic vaginitis may involve the use of topical estrogen or other estrogen replacement. To treat the symptoms, patients may use lubricants, but it may not help long term as it does not affect the tissues.
In a majority of postmenopausal women, there are risk factors that can contribute to atrophic vaginitis. Specifically, these risk factors are directly related to decreased estrogen levels and vaginal health. Some risk factors include
All of these factors impact estrogen levels and vaginal health, causing an increase in Atrophic vaginitis development.
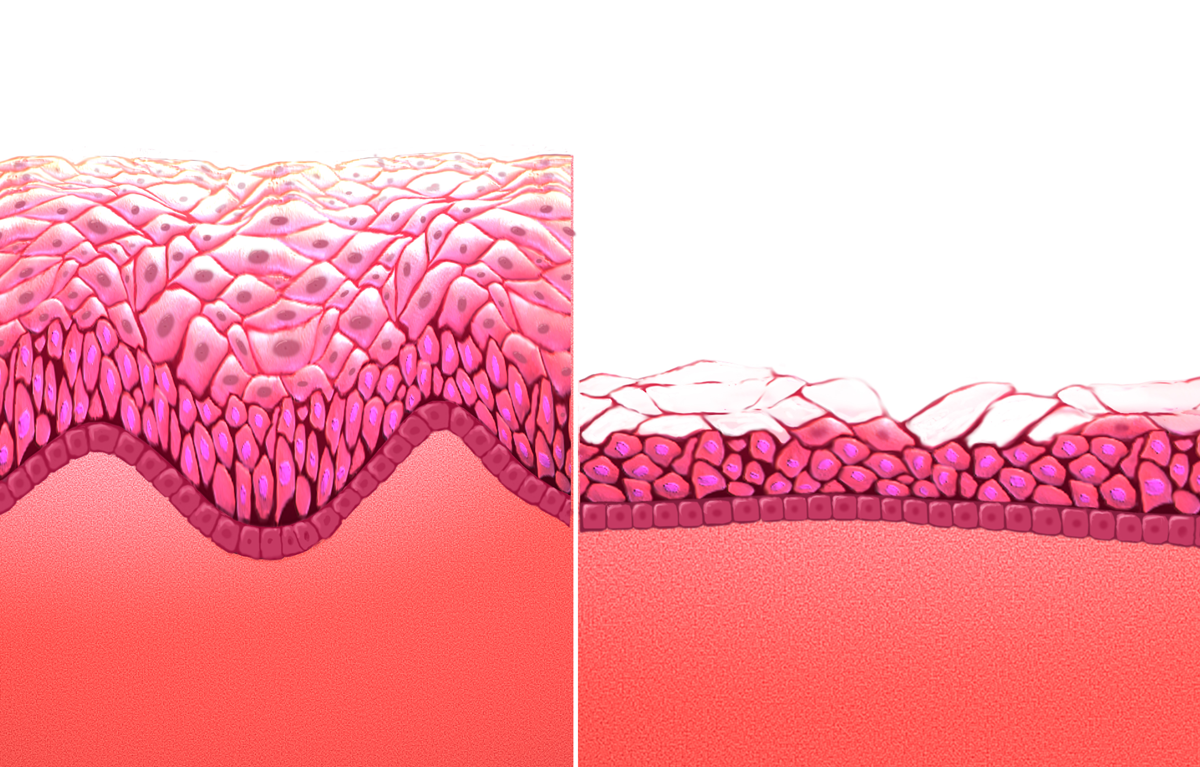
Atrophic vaginitis may be caused by tissue thinning, loss of elasticity, and loss of vaginal fluids from low estrogen levels. Normally, estrogen helps the vagina shed old cells, which are then converted into lactic acid by good bacteria. This keeps the vagina's pH acidic and healthy. When estrogen levels drop, this process slows down, leading to thinner vaginal tissue, less moisture, and a less acidic environment. As a result, there's a higher risk of getting vaginal and urinary tract infections. Normal menopause and treatments such as chemotherapy or medications may result in loss of estrogen.
Those with or had a history of breast cancer may be at a higher risk of developing atrophic vaginitis due to chemotherapy and other endocrine treatments. Estrogen is crucial for women's sexual and urinary health. It supports the tissues in the lower vagina and urinary tracts to keep them thick, elastic, and moist and ensuring good blood flow. Estrogen helps maintain a thick, glycogen-rich vaginal lining, which healthy bacteria use to produce lactic acid to keep the vaginal environment acidic, reducing infection risks. In premenopausal women, the main form of estrogen is called estradiol and fluctuates between 40 and 200 pg/mL, rising to 600 pg/mL during ovulation. Postmenopause, estrogen levels drop significantly tp 5-18 pg/mL, leading to gradual changes in the urogenital area. All tissue types such as connective, epithelial, muscular, blood vessels, and nerves are affected and become thinner and less effective, which increases risk of infections, inflammation, injuries, and sores. Blood flow and sensation can decrease, causing pain during sex and the pH level can rise due to decreased lactic acid production, which can allow harmful bacteria and fungi to grow and cause infections.
Antiestrogen medications may also contribute to the development of atrophic vaginitis. These medications include danazol, nafarelin, and medroxyprogesterone. Additional risk factors include smokers, those who have not given birth naturally (through the vagina), and increased prolactin levels while lactation.
Atrophic vaginitis
Atrophic vaginitis is inflammation of the vagina as a result of tissue thinning due to low estrogen levels. Symptoms may include pain during penetrative sex, vaginal itchiness or dryness, and an urge to urinate or burning with urination. It generally does not resolve without ongoing treatment. Complications may include urinary tract infections. Atrophic vaginitis as well as vulvovaginal atrophy, bladder and urethral dysfunctions are a group of conditions that constitute genitourinary syndrome of menopause (GSM). Diagnosis is typically based on symptoms.
The decrease in estrogen typically occurs following menopause. Other causes may include breastfeeding or using specific medications. Risk factors include smoking.
Treatment for atrophic vaginitis may involve the use of topical estrogen or other estrogen replacement. To treat the symptoms, patients may use lubricants, but it may not help long term as it does not affect the tissues.
In a majority of postmenopausal women, there are risk factors that can contribute to atrophic vaginitis. Specifically, these risk factors are directly related to decreased estrogen levels and vaginal health. Some risk factors include
All of these factors impact estrogen levels and vaginal health, causing an increase in Atrophic vaginitis development.
Atrophic vaginitis may be caused by tissue thinning, loss of elasticity, and loss of vaginal fluids from low estrogen levels. Normally, estrogen helps the vagina shed old cells, which are then converted into lactic acid by good bacteria. This keeps the vagina's pH acidic and healthy. When estrogen levels drop, this process slows down, leading to thinner vaginal tissue, less moisture, and a less acidic environment. As a result, there's a higher risk of getting vaginal and urinary tract infections. Normal menopause and treatments such as chemotherapy or medications may result in loss of estrogen.
Those with or had a history of breast cancer may be at a higher risk of developing atrophic vaginitis due to chemotherapy and other endocrine treatments. Estrogen is crucial for women's sexual and urinary health. It supports the tissues in the lower vagina and urinary tracts to keep them thick, elastic, and moist and ensuring good blood flow. Estrogen helps maintain a thick, glycogen-rich vaginal lining, which healthy bacteria use to produce lactic acid to keep the vaginal environment acidic, reducing infection risks. In premenopausal women, the main form of estrogen is called estradiol and fluctuates between 40 and 200 pg/mL, rising to 600 pg/mL during ovulation. Postmenopause, estrogen levels drop significantly tp 5-18 pg/mL, leading to gradual changes in the urogenital area. All tissue types such as connective, epithelial, muscular, blood vessels, and nerves are affected and become thinner and less effective, which increases risk of infections, inflammation, injuries, and sores. Blood flow and sensation can decrease, causing pain during sex and the pH level can rise due to decreased lactic acid production, which can allow harmful bacteria and fungi to grow and cause infections.
Antiestrogen medications may also contribute to the development of atrophic vaginitis. These medications include danazol, nafarelin, and medroxyprogesterone. Additional risk factors include smokers, those who have not given birth naturally (through the vagina), and increased prolactin levels while lactation.
Recent media
Recent media