Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Aortic stenosis
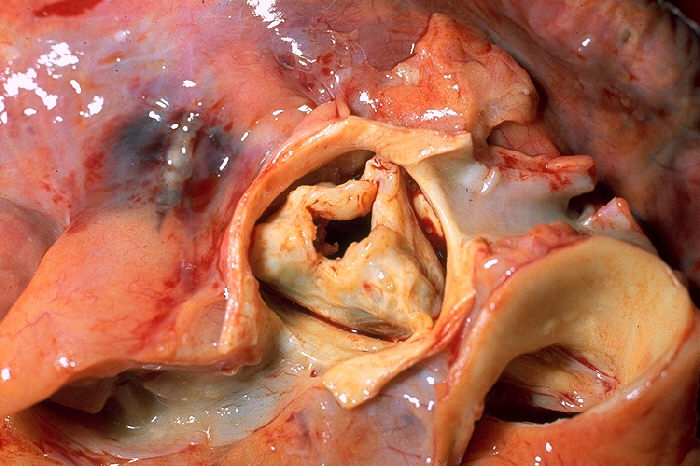
Aortic stenosis (AS or AoS) is the narrowing of the exit of the left ventricle of the heart (where the aorta begins), such that problems result. It may occur at the aortic valve as well as above and below this level. It typically gets worse over time. Symptoms often come on gradually, with a decreased ability to exercise often occurring first. If heart failure, loss of consciousness, or heart related chest pain occur due to AS the outcomes are worse. Loss of consciousness typically occurs with standing or exercising. Signs of heart failure include shortness of breath especially when lying down, at night, or with exercise, and swelling of the legs. Thickening of the valve without causing obstruction is known as aortic sclerosis.
Causes include being born with a bicuspid aortic valve, and rheumatic fever; a normal valve may also harden over the decades due to calcification. A bicuspid aortic valve affects about one to two percent of the population. As of 2014 rheumatic heart disease mostly occurs in the developing world. Risk factors are similar to those of coronary artery disease and include smoking, high blood pressure, high cholesterol, diabetes, and being male. The aortic valve usually has three leaflets and is located between the left ventricle of the heart and the aorta. AS typically results in a heart murmur. Its severity can be divided into mild, moderate, severe, and very severe, distinguishable by ultrasound scan of the heart.
Aortic stenosis is typically followed up with repeated ultrasound scans. Once it has become severe, treatment primarily involves valve replacement surgery, with transcatheter aortic valve replacement (TAVR) being an option in some who are at high risk from surgery. Valves may either be mechanical or bioprosthetic, with each having risks and benefits. Another less invasive procedure, balloon aortic valvuloplasty (BAV), may result in benefit, but for only a few months. Complications such as heart failure may be treated in the same way as in those with mild to moderate AS. In those with severe disease several medications should be avoided, including ACE inhibitors, nitroglycerin, and some beta blockers. Nitroprusside or phenylephrine may be used in those with decompensated heart failure depending on the blood pressure.
Aortic stenosis is the most common valvular heart disease in the developed world. It affects about 2% of people who are over 65 years of age. Estimated rates were not known in most of the developing world as of 2014. In those who have symptoms, without repair the chance of death at five years is about 50% and at 10 years is about 90%. Aortic stenosis was first described by French physician Lazare Rivière in 1663.
Symptoms related to aortic stenosis depend on the degree of stenosis. Most people with mild to moderate aortic stenosis do not have symptoms. Symptoms are usually present in individuals with severe aortic stenosis, though they may also occur in those with mild to moderate aortic stenosis. The three main symptoms of aortic stenosis are loss of consciousness, anginal chest pain and shortness of breath with activity or other symptoms of heart failure such as shortness of breath while lying flat, episodes of shortness of breath at night, or swollen legs and feet. It may also be accompanied by the characteristic "Dresden china" appearance of pallor with a light flush. [clarification needed]
Angina in the setting of heart failure also increases the risk of death. In people with angina, the 5-year mortality rate is 50% if the aortic valve is not replaced.
Angina in the setting of AS occurs due to left ventricular hypertrophy (LVH) that is caused by the constant production of increased pressure required to overcome the pressure gradient caused by the AS. While the muscular layer of the left ventricle thickens, the arteries that supply the muscle do not get significantly longer or bigger, so the muscle may not receive enough blood supply to meet its oxygen requirement. This ischemia may first be evident during exercise when the heart muscle requires increased blood supply to compensate for the increased workload. The individual may complain of anginal chest pain with exertion. Exercise stress testing with or without imaging is strictly contraindicated in symptomatic patients with severe aortic stenosis. Exercise stress test is now recommended by current guidelines in asymptomatic patients and may provide incremental prognostic value.
Eventually, however, the heart muscle will require more blood supply at rest than can be supplied by the coronary artery branches. At this point there may be signs of ventricular strain pattern (ST segment depression and T wave inversion) on the EKG, suggesting subendocardial ischemia. The subendocardium is the region that is most susceptible to ischemia because it is the most distant from the epicardial coronary arteries.
Hub AI
Aortic stenosis AI simulator
(@Aortic stenosis_simulator)
Aortic stenosis
Aortic stenosis (AS or AoS) is the narrowing of the exit of the left ventricle of the heart (where the aorta begins), such that problems result. It may occur at the aortic valve as well as above and below this level. It typically gets worse over time. Symptoms often come on gradually, with a decreased ability to exercise often occurring first. If heart failure, loss of consciousness, or heart related chest pain occur due to AS the outcomes are worse. Loss of consciousness typically occurs with standing or exercising. Signs of heart failure include shortness of breath especially when lying down, at night, or with exercise, and swelling of the legs. Thickening of the valve without causing obstruction is known as aortic sclerosis.
Causes include being born with a bicuspid aortic valve, and rheumatic fever; a normal valve may also harden over the decades due to calcification. A bicuspid aortic valve affects about one to two percent of the population. As of 2014 rheumatic heart disease mostly occurs in the developing world. Risk factors are similar to those of coronary artery disease and include smoking, high blood pressure, high cholesterol, diabetes, and being male. The aortic valve usually has three leaflets and is located between the left ventricle of the heart and the aorta. AS typically results in a heart murmur. Its severity can be divided into mild, moderate, severe, and very severe, distinguishable by ultrasound scan of the heart.
Aortic stenosis is typically followed up with repeated ultrasound scans. Once it has become severe, treatment primarily involves valve replacement surgery, with transcatheter aortic valve replacement (TAVR) being an option in some who are at high risk from surgery. Valves may either be mechanical or bioprosthetic, with each having risks and benefits. Another less invasive procedure, balloon aortic valvuloplasty (BAV), may result in benefit, but for only a few months. Complications such as heart failure may be treated in the same way as in those with mild to moderate AS. In those with severe disease several medications should be avoided, including ACE inhibitors, nitroglycerin, and some beta blockers. Nitroprusside or phenylephrine may be used in those with decompensated heart failure depending on the blood pressure.
Aortic stenosis is the most common valvular heart disease in the developed world. It affects about 2% of people who are over 65 years of age. Estimated rates were not known in most of the developing world as of 2014. In those who have symptoms, without repair the chance of death at five years is about 50% and at 10 years is about 90%. Aortic stenosis was first described by French physician Lazare Rivière in 1663.
Symptoms related to aortic stenosis depend on the degree of stenosis. Most people with mild to moderate aortic stenosis do not have symptoms. Symptoms are usually present in individuals with severe aortic stenosis, though they may also occur in those with mild to moderate aortic stenosis. The three main symptoms of aortic stenosis are loss of consciousness, anginal chest pain and shortness of breath with activity or other symptoms of heart failure such as shortness of breath while lying flat, episodes of shortness of breath at night, or swollen legs and feet. It may also be accompanied by the characteristic "Dresden china" appearance of pallor with a light flush. [clarification needed]
Angina in the setting of heart failure also increases the risk of death. In people with angina, the 5-year mortality rate is 50% if the aortic valve is not replaced.
Angina in the setting of AS occurs due to left ventricular hypertrophy (LVH) that is caused by the constant production of increased pressure required to overcome the pressure gradient caused by the AS. While the muscular layer of the left ventricle thickens, the arteries that supply the muscle do not get significantly longer or bigger, so the muscle may not receive enough blood supply to meet its oxygen requirement. This ischemia may first be evident during exercise when the heart muscle requires increased blood supply to compensate for the increased workload. The individual may complain of anginal chest pain with exertion. Exercise stress testing with or without imaging is strictly contraindicated in symptomatic patients with severe aortic stenosis. Exercise stress test is now recommended by current guidelines in asymptomatic patients and may provide incremental prognostic value.
Eventually, however, the heart muscle will require more blood supply at rest than can be supplied by the coronary artery branches. At this point there may be signs of ventricular strain pattern (ST segment depression and T wave inversion) on the EKG, suggesting subendocardial ischemia. The subendocardium is the region that is most susceptible to ischemia because it is the most distant from the epicardial coronary arteries.