Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
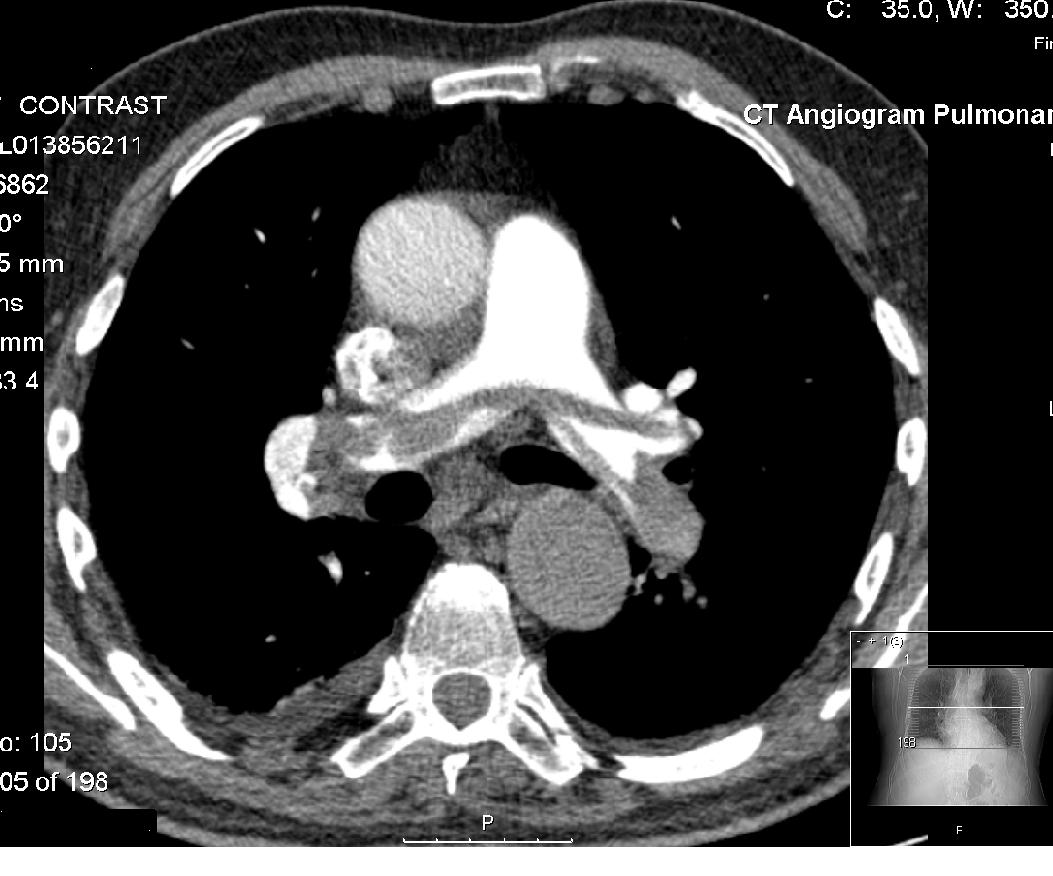
CT pulmonary angiogram
A CT pulmonary angiogram (CTPA) is a medical diagnostic test that employs computed tomography (CT) angiography to obtain an image of the pulmonary arteries. Its main use is to diagnose pulmonary embolism (PE). It is a preferred choice of imaging in the diagnosis of PE due to its minimally invasive nature for the patient, whose only requirement for the scan is an intravenous line.
Modern MDCT (multi-detector CT) scanners are able to deliver images of sufficient resolution within a short time period, such that CTPA has now supplanted previous methods of testing, such as direct pulmonary angiography, as the gold standard for diagnosis of pulmonary embolism.
The patient receives an intravenous injection of an iodine-containing contrast agent at a high rate using an injector pump. Images are acquired with the maximum intensity of radio-opaque contrast in the pulmonary arteries. This can be done using bolus tracking.
A normal CTPA scan will show the contrast filling the pulmonary vessels, appearing as bright white. Any mass filling defects, such as an embolus, will appear dark in place of the contrast, filling/blocking the space where blood should be flowing into the lungs.
CTPA was introduced in the 1990s as an alternative to ventilation/perfusion scanning (V/Q scan), which relies on radionuclide imaging of the blood vessels of the lung. It is regarded as a highly sensitive and specific test for pulmonary embolism.
CTPA is typically only requested if pulmonary embolism is suspected clinically. If the probability of PE is considered low, a blood test called D-dimer may be requested. If this is negative and risk of a PE is considered negligible, then CTPA or other scans are generally not performed. Most patients will have undergone a chest X-ray before CTPA is requested.
After initial concern that CTPA would miss smaller emboli, a 2007 study comparing CTPA directly with V/Q scanning found that CTPA identified more emboli without increasing the risk of long-term complications compared to V/Q scanning. A V/Q scan may still be recommended when a lower radiation dose is required.
On CTPA, acute emboli have been found at radiodensities ranging between about 5 and 65 Hounsfield units (HU), while chronic emboli have ranged between about 30 and 150.
Hub AI
CT pulmonary angiogram AI simulator
(@CT pulmonary angiogram_simulator)
CT pulmonary angiogram
A CT pulmonary angiogram (CTPA) is a medical diagnostic test that employs computed tomography (CT) angiography to obtain an image of the pulmonary arteries. Its main use is to diagnose pulmonary embolism (PE). It is a preferred choice of imaging in the diagnosis of PE due to its minimally invasive nature for the patient, whose only requirement for the scan is an intravenous line.
Modern MDCT (multi-detector CT) scanners are able to deliver images of sufficient resolution within a short time period, such that CTPA has now supplanted previous methods of testing, such as direct pulmonary angiography, as the gold standard for diagnosis of pulmonary embolism.
The patient receives an intravenous injection of an iodine-containing contrast agent at a high rate using an injector pump. Images are acquired with the maximum intensity of radio-opaque contrast in the pulmonary arteries. This can be done using bolus tracking.
A normal CTPA scan will show the contrast filling the pulmonary vessels, appearing as bright white. Any mass filling defects, such as an embolus, will appear dark in place of the contrast, filling/blocking the space where blood should be flowing into the lungs.
CTPA was introduced in the 1990s as an alternative to ventilation/perfusion scanning (V/Q scan), which relies on radionuclide imaging of the blood vessels of the lung. It is regarded as a highly sensitive and specific test for pulmonary embolism.
CTPA is typically only requested if pulmonary embolism is suspected clinically. If the probability of PE is considered low, a blood test called D-dimer may be requested. If this is negative and risk of a PE is considered negligible, then CTPA or other scans are generally not performed. Most patients will have undergone a chest X-ray before CTPA is requested.
After initial concern that CTPA would miss smaller emboli, a 2007 study comparing CTPA directly with V/Q scanning found that CTPA identified more emboli without increasing the risk of long-term complications compared to V/Q scanning. A V/Q scan may still be recommended when a lower radiation dose is required.
On CTPA, acute emboli have been found at radiodensities ranging between about 5 and 65 Hounsfield units (HU), while chronic emboli have ranged between about 30 and 150.