Recent from talks
Colorectal polyp
Knowledge base stats:
Talk channels stats:
Members stats:
Colorectal polyp
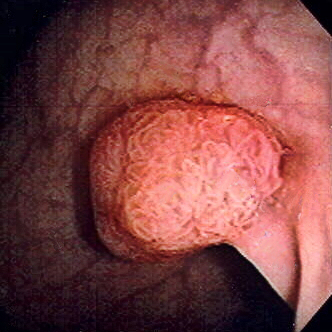
A colorectal polyp is a polyp (fleshy growth) occurring on the lining of the colon or rectum. Untreated colorectal polyps can develop into colorectal cancer.
Colorectal polyps are often classified by their behaviour (i.e. benign vs. malignant) or cause (e.g. as a consequence of inflammatory bowel disease). They may be benign (e.g. hyperplastic polyp), pre-malignant (e.g. tubular adenoma) or malignant (e.g. colorectal adenocarcinoma).
Colorectal polyps are not usually associated with symptoms. When they occur, symptoms include bloody stools; changes in frequency or consistency of stools (such as a week or more of constipation or diarrhoea); and fatigue arising from blood loss. Anemia arising from iron deficiency can also present due to chronic blood loss, even in the absence of bloody stools. Another symptom may be an increased mucus production especially those involving villous adenomas. Copious production of mucus causes loss of potassium that can occasionally result in symptomatic hypokalemia. Occasionally, if a polyp is big enough to cause a bowel obstruction, there may be nausea, vomiting and severe constipation.
Polyps are either pedunculated (attached to the intestinal wall by a stalk) or sessile (grow directly from the wall). In addition to the gross appearance categorization, they are further divided by their histologic appearance as tubular adenoma which are tubular glands, villous adenoma which are long finger like projections on the surface, and tubulovillous adenoma which has features of both.
Hereditary syndromes causing increased colorectal polyp formation include:
Several genes have been associated with polyposis, such as GREM1, MSH3, MLH3, NTHL1, RNF43 and RPS20.
Familial adenomatous polyposis (FAP) is a form of hereditary cancer syndrome involving the APC gene located on chromosome q521. The syndrome was first described in 1863 by Virchow on a 15-year-old boy with multiple polyps in his colon. The syndrome involves development of multiple polyps at an early age and those left untreated will all eventually develop cancer. The gene is expressed 100% in those with the mutation and it is autosomal dominant. 10–20% of patients have negative family history and acquire the syndrome from spontaneous germline mutation. The average age of newly diagnosed patient is 29 and the average age of newly discovered colorectal cancer is 39. It is recommended that those affected undergo colorectal cancer screening at younger age with treatment and prevention are surgical with removal of affected tissues.
Hereditary nonpolyposis colorectal cancer (HNPCC, also known as Lynch syndrome) is a hereditary colorectal cancer syndrome. It is the most common hereditary form of colorectal cancer in the United States and accounts for about 3% of all cases of cancer. It was first recognized by Alder S. Warthin in 1885 at the University of Michigan. It was later further studied by Henry Lynch who recognized an autosomal dominant transmission pattern with those affected having relatively early onset of cancer (mean age 44 years), greater occurrence of proximal lesions, mostly mucinous or poorly differentiated adenocarcinoma, greater number of synchronous and metachronous cancer cells, and good outcome after surgical intervention. The Amsterdam Criteria were initially used to define Lynch syndrome before the underlying genetic mechanism had been worked out. The Criteria required that the patient has three family members all first-degree relatives with colorectal cancer that involves at least two generations with at least one affected person being younger than 50 years of age when the diagnosis was made. The Amsterdam Criteria is too restrictive and was later expanded to include cancers of endometrial, ovarian, gastric, pancreatic, small intestinal, ureteral, and renal pelvic origin. The increased risk of cancer seen in patients with by the syndrome is associated with dysfunction of DNA repair mechanism. Molecular biologists have linked the syndrome to specific genes such as hMSH2, hMSH1, hMSH6, and hPMS2.
Hub AI
Colorectal polyp AI simulator
(@Colorectal polyp_simulator)
Colorectal polyp
A colorectal polyp is a polyp (fleshy growth) occurring on the lining of the colon or rectum. Untreated colorectal polyps can develop into colorectal cancer.
Colorectal polyps are often classified by their behaviour (i.e. benign vs. malignant) or cause (e.g. as a consequence of inflammatory bowel disease). They may be benign (e.g. hyperplastic polyp), pre-malignant (e.g. tubular adenoma) or malignant (e.g. colorectal adenocarcinoma).
Colorectal polyps are not usually associated with symptoms. When they occur, symptoms include bloody stools; changes in frequency or consistency of stools (such as a week or more of constipation or diarrhoea); and fatigue arising from blood loss. Anemia arising from iron deficiency can also present due to chronic blood loss, even in the absence of bloody stools. Another symptom may be an increased mucus production especially those involving villous adenomas. Copious production of mucus causes loss of potassium that can occasionally result in symptomatic hypokalemia. Occasionally, if a polyp is big enough to cause a bowel obstruction, there may be nausea, vomiting and severe constipation.
Polyps are either pedunculated (attached to the intestinal wall by a stalk) or sessile (grow directly from the wall). In addition to the gross appearance categorization, they are further divided by their histologic appearance as tubular adenoma which are tubular glands, villous adenoma which are long finger like projections on the surface, and tubulovillous adenoma which has features of both.
Hereditary syndromes causing increased colorectal polyp formation include:
Several genes have been associated with polyposis, such as GREM1, MSH3, MLH3, NTHL1, RNF43 and RPS20.
Familial adenomatous polyposis (FAP) is a form of hereditary cancer syndrome involving the APC gene located on chromosome q521. The syndrome was first described in 1863 by Virchow on a 15-year-old boy with multiple polyps in his colon. The syndrome involves development of multiple polyps at an early age and those left untreated will all eventually develop cancer. The gene is expressed 100% in those with the mutation and it is autosomal dominant. 10–20% of patients have negative family history and acquire the syndrome from spontaneous germline mutation. The average age of newly diagnosed patient is 29 and the average age of newly discovered colorectal cancer is 39. It is recommended that those affected undergo colorectal cancer screening at younger age with treatment and prevention are surgical with removal of affected tissues.
Hereditary nonpolyposis colorectal cancer (HNPCC, also known as Lynch syndrome) is a hereditary colorectal cancer syndrome. It is the most common hereditary form of colorectal cancer in the United States and accounts for about 3% of all cases of cancer. It was first recognized by Alder S. Warthin in 1885 at the University of Michigan. It was later further studied by Henry Lynch who recognized an autosomal dominant transmission pattern with those affected having relatively early onset of cancer (mean age 44 years), greater occurrence of proximal lesions, mostly mucinous or poorly differentiated adenocarcinoma, greater number of synchronous and metachronous cancer cells, and good outcome after surgical intervention. The Amsterdam Criteria were initially used to define Lynch syndrome before the underlying genetic mechanism had been worked out. The Criteria required that the patient has three family members all first-degree relatives with colorectal cancer that involves at least two generations with at least one affected person being younger than 50 years of age when the diagnosis was made. The Amsterdam Criteria is too restrictive and was later expanded to include cancers of endometrial, ovarian, gastric, pancreatic, small intestinal, ureteral, and renal pelvic origin. The increased risk of cancer seen in patients with by the syndrome is associated with dysfunction of DNA repair mechanism. Molecular biologists have linked the syndrome to specific genes such as hMSH2, hMSH1, hMSH6, and hPMS2.
Recent media