Recent from talks
HPV vaccine
Knowledge base stats:
Talk channels stats:
Members stats:
HPV vaccine
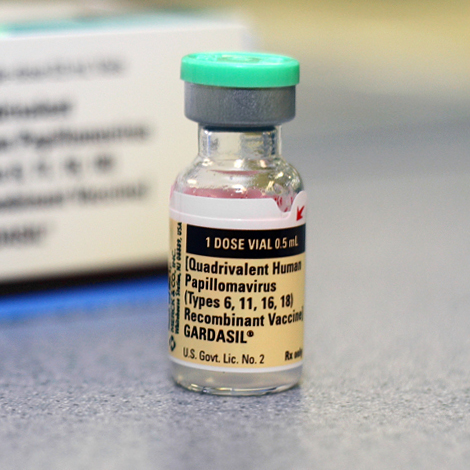
Human papillomavirus (HPV) vaccines are vaccines intended to provide acquired immunity against infection by certain types of human papillomavirus. The first HPV vaccine became available in 2006. Currently there are six licensed HPV vaccines: three bivalent (protect against two types of HPV), two quadrivalent (against four), and one nonavalent vaccine (against nine) All have excellent safety profiles and are highly efficacious, or have met immunobridging standards. All of them protect against HPV types 16 and 18, which are together responsible for approximately 70% of cervical cancer cases globally. The quadrivalent vaccines provide additional protection against HPV types 6 and 11. The nonavalent provides additional protection against HPV types 31, 33, 45, 52 and 58. It is estimated that HPV vaccines may prevent 70% of cervical cancer, 80% of anal cancer, 60% of vaginal cancer, 40% of vulvar cancer, and show more than 90% effectiveness in preventing HPV-positive oropharyngeal cancers. They also protect against penile cancer. They additionally prevent genital warts (also known as anogenital warts), with the quadrivalent and nonavalent vaccines providing virtually complete protection. The WHO recommends a one or two-dose schedule for girls aged 9–14 years, the same for girls and women aged 15–20 years, and two doses with a 6-month interval for women older than 21 years. The vaccines provide protection for at least five to ten years.
The primary target group in most of the countries recommending HPV vaccination is young adolescent girls, aged 9–14. The vaccination schedule depends on the age of the vaccine recipient. As of 2023, 27% of girls aged 9–14 years worldwide received at least one dose (37 countries were implementing the single-dose schedule, 45% of girls aged 9–14 years old vaccinated in that year). As of September 2024, 57 countries are implementing the single-dose schedule. At least 144 countries (at least 74% of WHO member states) provided the HPV vaccine in their national immunization schedule for girls, as of November 2024. As of 2022, 47 countries (24% of WHO member states) also did it for boys. Vaccinating a large portion of the population may also benefit the unvaccinated by way of herd immunity.
The HPV vaccine is on the World Health Organization's List of Essential Medicines. The World Health Organization (WHO) recommends HPV vaccines as part of routine vaccinations in all countries, along with other prevention measures. The WHO's priority purpose of HPV immunization is the prevention of cervical cancer, which accounts for 82% of all HPV-related cancers and more than 95% of which are caused by HPV. 88% (2020 figure) of cervical cancers and 90% of deaths occur in low- and middle-income countries and 2% (2020 figure) in high-income countries. The WHO-recommended primary target population for HPV vaccination is girls aged 9–14 years before they become sexually active. It aims the introduction of the HPV vaccine in all countries and has set a target of reaching a coverage of 90% of girls fully vaccinated with HPV vaccine by age 15 years. Females aged ≥15 years, boys, older males or men who have sex with men (MSM) are secondary target populations. HPV vaccination is the most cost-effective public health measure against cervical cancer, particularly in resource-constrained settings. Cervical cancer screening is still required following vaccination.
The WHO recommends a one or two-dose schedule for girls aged 9–14 years, the same for girls and women aged 15–20 years, and two doses with a 6-month interval for women older than 21 years. A one-or-two-dose schedule is also used in boys and men aged 9–20 years, though WHO makes no specific recommendation for males. WHO has prequalified a total of 6 kinds of vaccines. Among these, Cecolin (bivalent), Cervarix, Gardasil (quadrivalent) and Gardasil 9 (nonavalent) are confirmed for use in a single-dose schedule. The remaining vaccine, Walrinvax (bivalent), is only prequalified for two-dose schedule for now (as of October 2024[update]).
The single-dose schedule is a recent (circa 2022) development based on studies on girls and women showing a similar level and duration of protection when taking one dose instead of two. It is a form of off-label use. In 2025, a randomized trial’s 5-year extension reported that among Tanzanian girls vaccinated at ages 9–14, ≥99% remained seropositive for HPV-16 and 93–98% for HPV-18 at month 60 after a single dose, while antibody concentrations were stable from months 12–60. Not much is known about the efficacy and protective duration of the simplified schedule in boys and men.
The large majority of cervical cancer cases in 2020 (88%) occurred in LMICs, where they account for 17% of all cancers in women, compared with only 2% in high-income countries (HICs). In sub-Saharan Africa, the region with the highest rates of young WLWH, approximately 20% of cervical cancer cases occur in WLWH [women living with HIV]. HPV infection is more likely to persist and to progress to cancer in WLWH.33 Mortality rates vary 50-fold between countries, ranging from <2 per 100 000 women in some HICs to >40 per 100 000 in some countries of sub-Saharan Africa.
Of the 20 hardest hit countries by cervical cancer, 19 are in Africa.
The US National Cancer Institute states "Widespread vaccination has the potential to reduce cervical cancer deaths around the world by as much as two-thirds if all women were to take the vaccine and if protection turns out to be long-term. In addition, the vaccines can reduce the need for medical care, biopsies, and invasive procedures associated with the follow-up from abnormal Pap tests, thus helping to reduce health care costs and anxieties related to abnormal Pap tests and follow-up procedures."
Hub AI
HPV vaccine AI simulator
(@HPV vaccine_simulator)
HPV vaccine
Human papillomavirus (HPV) vaccines are vaccines intended to provide acquired immunity against infection by certain types of human papillomavirus. The first HPV vaccine became available in 2006. Currently there are six licensed HPV vaccines: three bivalent (protect against two types of HPV), two quadrivalent (against four), and one nonavalent vaccine (against nine) All have excellent safety profiles and are highly efficacious, or have met immunobridging standards. All of them protect against HPV types 16 and 18, which are together responsible for approximately 70% of cervical cancer cases globally. The quadrivalent vaccines provide additional protection against HPV types 6 and 11. The nonavalent provides additional protection against HPV types 31, 33, 45, 52 and 58. It is estimated that HPV vaccines may prevent 70% of cervical cancer, 80% of anal cancer, 60% of vaginal cancer, 40% of vulvar cancer, and show more than 90% effectiveness in preventing HPV-positive oropharyngeal cancers. They also protect against penile cancer. They additionally prevent genital warts (also known as anogenital warts), with the quadrivalent and nonavalent vaccines providing virtually complete protection. The WHO recommends a one or two-dose schedule for girls aged 9–14 years, the same for girls and women aged 15–20 years, and two doses with a 6-month interval for women older than 21 years. The vaccines provide protection for at least five to ten years.
The primary target group in most of the countries recommending HPV vaccination is young adolescent girls, aged 9–14. The vaccination schedule depends on the age of the vaccine recipient. As of 2023, 27% of girls aged 9–14 years worldwide received at least one dose (37 countries were implementing the single-dose schedule, 45% of girls aged 9–14 years old vaccinated in that year). As of September 2024, 57 countries are implementing the single-dose schedule. At least 144 countries (at least 74% of WHO member states) provided the HPV vaccine in their national immunization schedule for girls, as of November 2024. As of 2022, 47 countries (24% of WHO member states) also did it for boys. Vaccinating a large portion of the population may also benefit the unvaccinated by way of herd immunity.
The HPV vaccine is on the World Health Organization's List of Essential Medicines. The World Health Organization (WHO) recommends HPV vaccines as part of routine vaccinations in all countries, along with other prevention measures. The WHO's priority purpose of HPV immunization is the prevention of cervical cancer, which accounts for 82% of all HPV-related cancers and more than 95% of which are caused by HPV. 88% (2020 figure) of cervical cancers and 90% of deaths occur in low- and middle-income countries and 2% (2020 figure) in high-income countries. The WHO-recommended primary target population for HPV vaccination is girls aged 9–14 years before they become sexually active. It aims the introduction of the HPV vaccine in all countries and has set a target of reaching a coverage of 90% of girls fully vaccinated with HPV vaccine by age 15 years. Females aged ≥15 years, boys, older males or men who have sex with men (MSM) are secondary target populations. HPV vaccination is the most cost-effective public health measure against cervical cancer, particularly in resource-constrained settings. Cervical cancer screening is still required following vaccination.
The WHO recommends a one or two-dose schedule for girls aged 9–14 years, the same for girls and women aged 15–20 years, and two doses with a 6-month interval for women older than 21 years. A one-or-two-dose schedule is also used in boys and men aged 9–20 years, though WHO makes no specific recommendation for males. WHO has prequalified a total of 6 kinds of vaccines. Among these, Cecolin (bivalent), Cervarix, Gardasil (quadrivalent) and Gardasil 9 (nonavalent) are confirmed for use in a single-dose schedule. The remaining vaccine, Walrinvax (bivalent), is only prequalified for two-dose schedule for now (as of October 2024[update]).
The single-dose schedule is a recent (circa 2022) development based on studies on girls and women showing a similar level and duration of protection when taking one dose instead of two. It is a form of off-label use. In 2025, a randomized trial’s 5-year extension reported that among Tanzanian girls vaccinated at ages 9–14, ≥99% remained seropositive for HPV-16 and 93–98% for HPV-18 at month 60 after a single dose, while antibody concentrations were stable from months 12–60. Not much is known about the efficacy and protective duration of the simplified schedule in boys and men.
The large majority of cervical cancer cases in 2020 (88%) occurred in LMICs, where they account for 17% of all cancers in women, compared with only 2% in high-income countries (HICs). In sub-Saharan Africa, the region with the highest rates of young WLWH, approximately 20% of cervical cancer cases occur in WLWH [women living with HIV]. HPV infection is more likely to persist and to progress to cancer in WLWH.33 Mortality rates vary 50-fold between countries, ranging from <2 per 100 000 women in some HICs to >40 per 100 000 in some countries of sub-Saharan Africa.
Of the 20 hardest hit countries by cervical cancer, 19 are in Africa.
The US National Cancer Institute states "Widespread vaccination has the potential to reduce cervical cancer deaths around the world by as much as two-thirds if all women were to take the vaccine and if protection turns out to be long-term. In addition, the vaccines can reduce the need for medical care, biopsies, and invasive procedures associated with the follow-up from abnormal Pap tests, thus helping to reduce health care costs and anxieties related to abnormal Pap tests and follow-up procedures."
Recent media