Recent from talks
Herpes simplex virus
Knowledge base stats:
Talk channels stats:
Members stats:
Herpes simplex virus
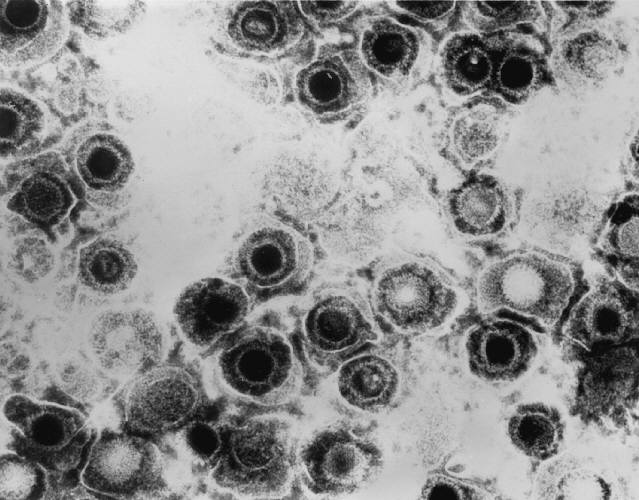
Herpes simplex virus 1 and 2 (HSV-1 and HSV-2) are two members of the human Herpesviridae family, a set of viruses that produce viral infections in the majority of humans. Both HSV-1 and HSV-2 are very common and contagious. They can be spread when an infected person begins shedding the virus.
As of 2016, about 67% of the world population under the age of 50 had HSV-1. In the United States, about 47.8% and 11.9% are estimated to have HSV-1 and HSV-2, respectively, though actual prevalence may be much higher. Because it can be transmitted through any intimate contact, it is one of the most common sexually transmitted infections.
Many of those who are infected never develop symptoms. Symptoms, when they occur, may include watery blisters in the skin of any location of the body, or in mucous membranes of the mouth, lips, nose, genitals, or eyes (herpes simplex keratitis). Lesions heal with a scab characteristic of herpetic disease. Sometimes, the viruses cause mild or atypical symptoms during outbreaks. However, they can also cause more troublesome forms of herpes simplex. As neurotropic and neuroinvasive viruses, HSV-1 and -2 persist in the body by hiding from the immune system in the cell bodies of neurons, particularly in sensory ganglia. After the initial or primary infection, some infected people experience sporadic episodes of viral reactivation or outbreaks. In an outbreak, the virus in a nerve cell becomes active and is transported via the neuron's axon to the skin, where virus replication and shedding occur and may cause new sores.
HSV-1 and HSV-2 are transmitted by contact with an infected person who has reactivations of the virus. HSV 1 and HSV-2 are periodically shed, most often asymptomatically. [citation needed]
In a study of people with first-episode genital HSV-1 infection from 2022, genital shedding of HSV-1 was detected on 12% of days at 2 months and declined significantly to 7% of days at 11 months. Most genital shedding was asymptomatic; genital and oral lesions and oral shedding were rare.
Most sexual transmissions of HSV-2 occur during periods of asymptomatic shedding. Asymptomatic reactivation means that the virus causes atypical, subtle, or hard-to-notice symptoms that are not identified as an active herpes infection, so acquiring the virus is possible even if no active HSV blisters or sores are present. In one study, daily genital swab samples detected HSV-2 at a median of 12–28% of days among those who had an outbreak, and 10% of days among those with asymptomatic infection (no prior outbreaks), with many of these episodes occurring without visible outbreak ("subclinical shedding").
In another study, 73 subjects were randomized to receive valaciclovir 1 g daily or placebo for 60 days each in a two-way crossover design. A daily swab of the genital area was self-collected for HSV-2 detection by polymerase chain reaction, to compare the effect of valaciclovir versus placebo on asymptomatic viral shedding in immunocompetent, HSV-2 seropositive subjects without a history of symptomatic genital herpes infection. The study found that valaciclovir significantly reduced shedding during subclinical days compared to placebo, showing a 71% reduction; 84% of subjects had no shedding while receiving valaciclovir versus 54% of subjects on placebo. About 88% of patients treated with valaciclovir had no recognized signs or symptoms versus 77% for placebo.
For HSV-2, subclinical shedding may account for most of the transmission. Studies on discordant partners (one infected with HSV-2, one not) show that the transmission rate is approximately 5–8.9 per 10,000 sexual contacts, with condom usage greatly reducing the risk of acquisition. Atypical symptoms are often attributed to other causes, such as a yeast infection. HSV-1 is often acquired orally during childhood. It may also be sexually transmitted, including contact with saliva, such as kissing and oral sex. Historically HSV-2 was primarily a sexually transmitted infection, but rates of HSV-1 genital infections have been increasing for the last few decades.
Hub AI
Herpes simplex virus AI simulator
(@Herpes simplex virus_simulator)
Herpes simplex virus
Herpes simplex virus 1 and 2 (HSV-1 and HSV-2) are two members of the human Herpesviridae family, a set of viruses that produce viral infections in the majority of humans. Both HSV-1 and HSV-2 are very common and contagious. They can be spread when an infected person begins shedding the virus.
As of 2016, about 67% of the world population under the age of 50 had HSV-1. In the United States, about 47.8% and 11.9% are estimated to have HSV-1 and HSV-2, respectively, though actual prevalence may be much higher. Because it can be transmitted through any intimate contact, it is one of the most common sexually transmitted infections.
Many of those who are infected never develop symptoms. Symptoms, when they occur, may include watery blisters in the skin of any location of the body, or in mucous membranes of the mouth, lips, nose, genitals, or eyes (herpes simplex keratitis). Lesions heal with a scab characteristic of herpetic disease. Sometimes, the viruses cause mild or atypical symptoms during outbreaks. However, they can also cause more troublesome forms of herpes simplex. As neurotropic and neuroinvasive viruses, HSV-1 and -2 persist in the body by hiding from the immune system in the cell bodies of neurons, particularly in sensory ganglia. After the initial or primary infection, some infected people experience sporadic episodes of viral reactivation or outbreaks. In an outbreak, the virus in a nerve cell becomes active and is transported via the neuron's axon to the skin, where virus replication and shedding occur and may cause new sores.
HSV-1 and HSV-2 are transmitted by contact with an infected person who has reactivations of the virus. HSV 1 and HSV-2 are periodically shed, most often asymptomatically. [citation needed]
In a study of people with first-episode genital HSV-1 infection from 2022, genital shedding of HSV-1 was detected on 12% of days at 2 months and declined significantly to 7% of days at 11 months. Most genital shedding was asymptomatic; genital and oral lesions and oral shedding were rare.
Most sexual transmissions of HSV-2 occur during periods of asymptomatic shedding. Asymptomatic reactivation means that the virus causes atypical, subtle, or hard-to-notice symptoms that are not identified as an active herpes infection, so acquiring the virus is possible even if no active HSV blisters or sores are present. In one study, daily genital swab samples detected HSV-2 at a median of 12–28% of days among those who had an outbreak, and 10% of days among those with asymptomatic infection (no prior outbreaks), with many of these episodes occurring without visible outbreak ("subclinical shedding").
In another study, 73 subjects were randomized to receive valaciclovir 1 g daily or placebo for 60 days each in a two-way crossover design. A daily swab of the genital area was self-collected for HSV-2 detection by polymerase chain reaction, to compare the effect of valaciclovir versus placebo on asymptomatic viral shedding in immunocompetent, HSV-2 seropositive subjects without a history of symptomatic genital herpes infection. The study found that valaciclovir significantly reduced shedding during subclinical days compared to placebo, showing a 71% reduction; 84% of subjects had no shedding while receiving valaciclovir versus 54% of subjects on placebo. About 88% of patients treated with valaciclovir had no recognized signs or symptoms versus 77% for placebo.
For HSV-2, subclinical shedding may account for most of the transmission. Studies on discordant partners (one infected with HSV-2, one not) show that the transmission rate is approximately 5–8.9 per 10,000 sexual contacts, with condom usage greatly reducing the risk of acquisition. Atypical symptoms are often attributed to other causes, such as a yeast infection. HSV-1 is often acquired orally during childhood. It may also be sexually transmitted, including contact with saliva, such as kissing and oral sex. Historically HSV-2 was primarily a sexually transmitted infection, but rates of HSV-1 genital infections have been increasing for the last few decades.
Recent media