
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Intraventricular hemorrhage AI simulator
(@Intraventricular hemorrhage_simulator)
Hub AI
Intraventricular hemorrhage AI simulator
(@Intraventricular hemorrhage_simulator)
Intraventricular hemorrhage
Intraventricular hemorrhage (IVH), also known as intraventricular bleeding, is a bleeding into the brain's ventricular system, where the cerebrospinal fluid is produced and circulates through towards the subarachnoid space. It can result from physical trauma or from hemorrhagic stroke.
30% of intraventricular hemorrhage (IVH) are primary, confined to the ventricular system and typically caused by intraventricular trauma, aneurysm, vascular malformations, or tumors, particularly of the choroid plexus. However 70% of IVH are secondary in nature, resulting from an expansion of an existing intraparenchymal or subarachnoid hemorrhage. Intraventricular hemorrhage has been found to occur in 35% of moderate to severe traumatic brain injuries. Thus the hemorrhage usually does not occur without extensive associated damage, and so the outcome is rarely good.
Symptoms of IVH are similar to other intracerebral hemorrhages and include sudden onset of headache, nausea and vomiting, together with an alteration of the mental state and/or level of consciousness. Focal neurological signs that affect specific regions of the body are either minimal or absent, but focal and/or generalized seizures may occur. Xanthochromia, yellow-tinged cerebral spinal fluid, is a common finding, however other medical conditions can also be associated with xanthochromia.
Some infants are asymptomatic and others may present with hard to detect abnormalities of consciousness, muscle tone, breathing, movements of their eyes, and body movements.
Causes of IVH in adults include physical trauma or from hemorrhagic stroke.
Infants that are preterm and very low birth weight are also at high risk. IVH in the preterm brain usually arises from the germinal matrix whereas IVH in the term infants originates from the choroid plexus. However, it is particularly common in premature infants or those of very low birth weight. The cause of IVH in premature infants, unlike that in older infants, children or adults, is rarely due to trauma. Instead it is thought to result from changes in perfusion of the delicate cellular structures that are present in the growing brain, augmented by the immaturity of the cerebral circulatory system, which is especially vulnerable to hypoxic ischemic encephalopathy. The lack of blood flow results in cell death and subsequent breakdown of the blood vessel walls, leading to bleeding. While this bleeding can result in further injury, it is itself a marker for injury that has already occurred. Most intraventricular hemorrhages occur in the first 72 hours after birth. The risk is increased with use of extracorporeal membrane oxygenation in preterm infants. Congenital cytomegalovirus infection can be an important cause.
The most common cause for periventricular-intraventricular hemorrhage (PIVH) in newborn infants is the fragility and unique morphology of blood vessels in the germinal matrix, as well as an immature cerebral autoregulation mechanism. This mechanism normally allows the brain to maintain stable blood flow despite blood pressure fluctuations, so underdevelopment in this area markedly increases the risk of bleeding. In addition, blood vessels in the neonatal germinal matrix have a higher density, surface area, and rounder shape. These differences further contribute to IVH risk. Some external risk factors of neonatal IVH include transport following outside delivery, mechanical ventilation, and frequent intubation.
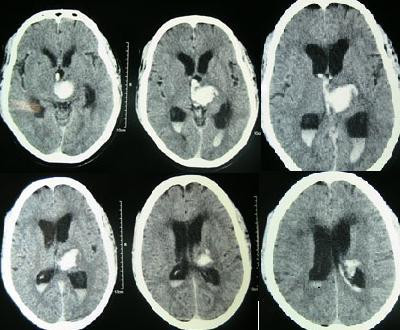
Diagnosis can be confirmed by the presence of blood inside the ventricles on CT.
Intraventricular hemorrhage
Intraventricular hemorrhage (IVH), also known as intraventricular bleeding, is a bleeding into the brain's ventricular system, where the cerebrospinal fluid is produced and circulates through towards the subarachnoid space. It can result from physical trauma or from hemorrhagic stroke.
30% of intraventricular hemorrhage (IVH) are primary, confined to the ventricular system and typically caused by intraventricular trauma, aneurysm, vascular malformations, or tumors, particularly of the choroid plexus. However 70% of IVH are secondary in nature, resulting from an expansion of an existing intraparenchymal or subarachnoid hemorrhage. Intraventricular hemorrhage has been found to occur in 35% of moderate to severe traumatic brain injuries. Thus the hemorrhage usually does not occur without extensive associated damage, and so the outcome is rarely good.
Symptoms of IVH are similar to other intracerebral hemorrhages and include sudden onset of headache, nausea and vomiting, together with an alteration of the mental state and/or level of consciousness. Focal neurological signs that affect specific regions of the body are either minimal or absent, but focal and/or generalized seizures may occur. Xanthochromia, yellow-tinged cerebral spinal fluid, is a common finding, however other medical conditions can also be associated with xanthochromia.
Some infants are asymptomatic and others may present with hard to detect abnormalities of consciousness, muscle tone, breathing, movements of their eyes, and body movements.
Causes of IVH in adults include physical trauma or from hemorrhagic stroke.
Infants that are preterm and very low birth weight are also at high risk. IVH in the preterm brain usually arises from the germinal matrix whereas IVH in the term infants originates from the choroid plexus. However, it is particularly common in premature infants or those of very low birth weight. The cause of IVH in premature infants, unlike that in older infants, children or adults, is rarely due to trauma. Instead it is thought to result from changes in perfusion of the delicate cellular structures that are present in the growing brain, augmented by the immaturity of the cerebral circulatory system, which is especially vulnerable to hypoxic ischemic encephalopathy. The lack of blood flow results in cell death and subsequent breakdown of the blood vessel walls, leading to bleeding. While this bleeding can result in further injury, it is itself a marker for injury that has already occurred. Most intraventricular hemorrhages occur in the first 72 hours after birth. The risk is increased with use of extracorporeal membrane oxygenation in preterm infants. Congenital cytomegalovirus infection can be an important cause.
The most common cause for periventricular-intraventricular hemorrhage (PIVH) in newborn infants is the fragility and unique morphology of blood vessels in the germinal matrix, as well as an immature cerebral autoregulation mechanism. This mechanism normally allows the brain to maintain stable blood flow despite blood pressure fluctuations, so underdevelopment in this area markedly increases the risk of bleeding. In addition, blood vessels in the neonatal germinal matrix have a higher density, surface area, and rounder shape. These differences further contribute to IVH risk. Some external risk factors of neonatal IVH include transport following outside delivery, mechanical ventilation, and frequent intubation.
Diagnosis can be confirmed by the presence of blood inside the ventricles on CT.
Recent media
Recent media