Recent from talks
Neuronal ceroid lipofuscinosis
Knowledge base stats:
Talk channels stats:
Members stats:
Neuronal ceroid lipofuscinosis
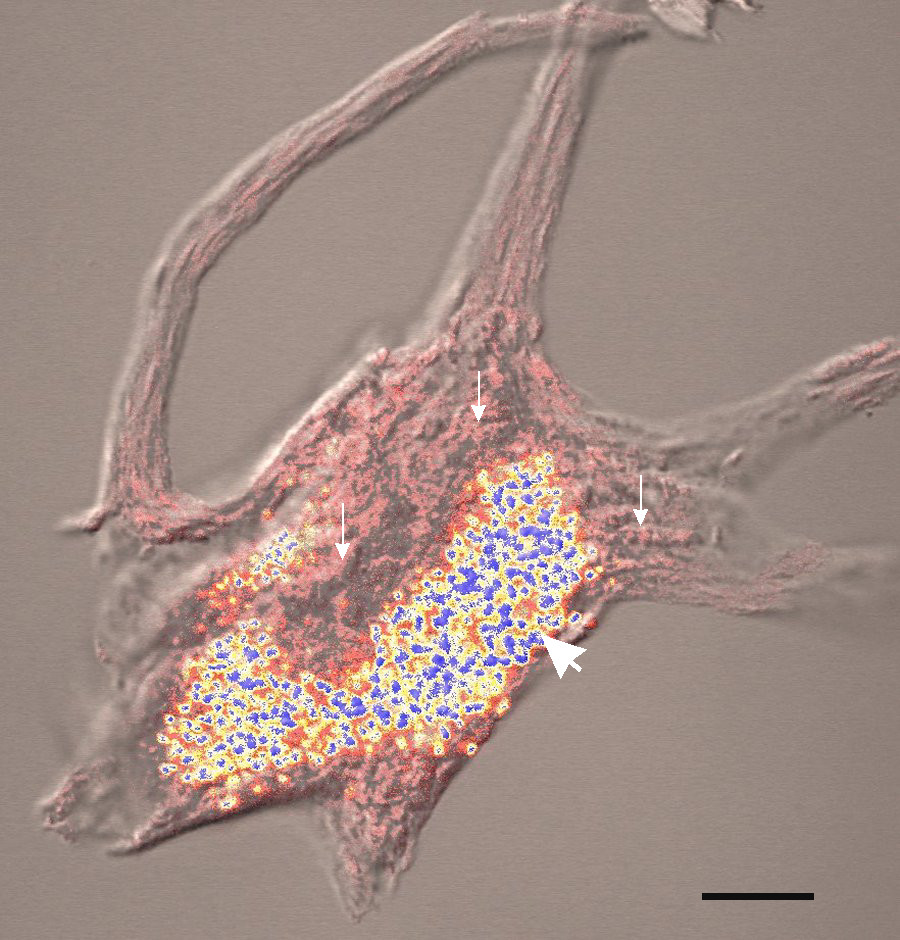
Neuronal ceroid lipofuscinosis is a family of at least eight genetically separate neurodegenerative lysosomal storage diseases that result from excessive accumulation of lipopigments (lipofuscin) in the body's tissues. These lipopigments are made up of fats and proteins. Their name comes from the word stem "lipo-", which is a variation on lipid, and from the term "pigment", used because the substances take on a greenish-yellow color when viewed under an ultraviolet light microscope. These lipofuscin materials build up in neuronal cells and many organs, including the liver, spleen, myocardium, and kidneys.
The classic characterization of the group of neurodegenerative, lysosomal storage disorders called the neuronal ceroid lipofuscinoses (NCLs) is through the progressive, permanent loss of motor and psychological ability with a severe intracellular accumulation of lipofuscins, with the United States and Northern European populations having slightly higher frequency with an occurrence of one in 10,000. Four classic diagnoses have received the most attention from researchers and the medical field, differentiated from one another by age of symptomatic onset, duration, early-onset manifestations such as blindness or seizures, and the forms which lipofuscin accumulation takes.
In the early infantile variant of NCL (also called INCL or Santavuori-Haltia), probands appear normal at birth, but early visual loss leading to complete retinal blindness by the age of 2 years is the first indicator of the disease; by 3 years of age, a vegetative state is reached, and by 4 years, isoelectric encephalograms confirm brain death. Late infantile variant usually manifests between 2 and 4 years of age with seizures and deterioration of vision. The maximum age before death for late infantile variant is 10–12 years. Juvenile NCL (JNCL, Batten disease, or Spielmeyer-Vogt), with a prevalence of one in 100,000, usually arises between 4 and 10 years of age; the first symptoms include considerable vision loss due to retinal dystrophy, with seizures, psychological degeneration, and eventual death in the mid- to late 20s or 30s ensuing. Adult variant NCL (ANCL or Kuf's disease) is less understood and generally manifests milder symptoms; however, while symptoms typically appear around 30 years of age, death usually occurs 10 years later.
All the mutations that have been associated with this disease have been linked to genes involved with the neural synapses metabolism – most commonly with the reuse of vesicle proteins.[citation needed]
Childhood NCLs are generally autosomal recessive disorders; that is, they occur only when a child inherits two copies of the defective gene, one from each parent. When both parents carry one defective gene, each of their children faces a one in four chance of developing NCL. At the same time, each child also faces a one in two chance of inheriting just one copy of the defective gene. Individuals who have only one defective gene are known as carriers, meaning they do not develop the disease, but they can pass the gene on to their own children. The most commonly identified mutations are in the CLN3 gene, which is located on the short arm of chromosome 16 (16p12.1). The normal function of the gene is not presently known, but results in a transmembrane protein.[citation needed]
Adult NCL may be inherited as an autosomal recessive (Kufs), or less often, as an autosomal dominant (Parry's) disorder. In autosomal dominant inheritance, all people who inherit a single copy of the disease gene develop the disease. As a result, no carriers of the gene are unaffected.[citation needed]
Many authorities refer to the NCLs collectively as Batten disease.
Because vision loss is often an early sign, NCL may be first suspected during an eye exam. An eye doctor can detect a loss of cells within the eye that occurs in the three childhood forms of NCL. However, because such cell loss occurs in other eye diseases, the disorder cannot be diagnosed by this sign alone. Often, an eye specialist or other physician who suspects NCL may refer the child to a neurologist, a doctor who specializes in disease of the brain and nervous system. To diagnose NCL, the neurologist needs the patient's medical history and information from various laboratory tests.[citation needed]
Hub AI
Neuronal ceroid lipofuscinosis AI simulator
(@Neuronal ceroid lipofuscinosis_simulator)
Neuronal ceroid lipofuscinosis
Neuronal ceroid lipofuscinosis is a family of at least eight genetically separate neurodegenerative lysosomal storage diseases that result from excessive accumulation of lipopigments (lipofuscin) in the body's tissues. These lipopigments are made up of fats and proteins. Their name comes from the word stem "lipo-", which is a variation on lipid, and from the term "pigment", used because the substances take on a greenish-yellow color when viewed under an ultraviolet light microscope. These lipofuscin materials build up in neuronal cells and many organs, including the liver, spleen, myocardium, and kidneys.
The classic characterization of the group of neurodegenerative, lysosomal storage disorders called the neuronal ceroid lipofuscinoses (NCLs) is through the progressive, permanent loss of motor and psychological ability with a severe intracellular accumulation of lipofuscins, with the United States and Northern European populations having slightly higher frequency with an occurrence of one in 10,000. Four classic diagnoses have received the most attention from researchers and the medical field, differentiated from one another by age of symptomatic onset, duration, early-onset manifestations such as blindness or seizures, and the forms which lipofuscin accumulation takes.
In the early infantile variant of NCL (also called INCL or Santavuori-Haltia), probands appear normal at birth, but early visual loss leading to complete retinal blindness by the age of 2 years is the first indicator of the disease; by 3 years of age, a vegetative state is reached, and by 4 years, isoelectric encephalograms confirm brain death. Late infantile variant usually manifests between 2 and 4 years of age with seizures and deterioration of vision. The maximum age before death for late infantile variant is 10–12 years. Juvenile NCL (JNCL, Batten disease, or Spielmeyer-Vogt), with a prevalence of one in 100,000, usually arises between 4 and 10 years of age; the first symptoms include considerable vision loss due to retinal dystrophy, with seizures, psychological degeneration, and eventual death in the mid- to late 20s or 30s ensuing. Adult variant NCL (ANCL or Kuf's disease) is less understood and generally manifests milder symptoms; however, while symptoms typically appear around 30 years of age, death usually occurs 10 years later.
All the mutations that have been associated with this disease have been linked to genes involved with the neural synapses metabolism – most commonly with the reuse of vesicle proteins.[citation needed]
Childhood NCLs are generally autosomal recessive disorders; that is, they occur only when a child inherits two copies of the defective gene, one from each parent. When both parents carry one defective gene, each of their children faces a one in four chance of developing NCL. At the same time, each child also faces a one in two chance of inheriting just one copy of the defective gene. Individuals who have only one defective gene are known as carriers, meaning they do not develop the disease, but they can pass the gene on to their own children. The most commonly identified mutations are in the CLN3 gene, which is located on the short arm of chromosome 16 (16p12.1). The normal function of the gene is not presently known, but results in a transmembrane protein.[citation needed]
Adult NCL may be inherited as an autosomal recessive (Kufs), or less often, as an autosomal dominant (Parry's) disorder. In autosomal dominant inheritance, all people who inherit a single copy of the disease gene develop the disease. As a result, no carriers of the gene are unaffected.[citation needed]
Many authorities refer to the NCLs collectively as Batten disease.
Because vision loss is often an early sign, NCL may be first suspected during an eye exam. An eye doctor can detect a loss of cells within the eye that occurs in the three childhood forms of NCL. However, because such cell loss occurs in other eye diseases, the disorder cannot be diagnosed by this sign alone. Often, an eye specialist or other physician who suspects NCL may refer the child to a neurologist, a doctor who specializes in disease of the brain and nervous system. To diagnose NCL, the neurologist needs the patient's medical history and information from various laboratory tests.[citation needed]
Recent media