Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Obstetrical forceps
Obstetrical forceps are a medical instrument used in childbirth. Their use can serve as an alternative to the ventouse (vacuum extraction) method.
Forceps births, like all assisted births, should be undertaken only to help promote the health of the mother or baby. In general, a forceps birth is likely to be safer for both the mother and baby than the alternatives – either a ventouse birth or a caesarean section – although caveats such as operator skill apply.
Advantages of forceps use include avoidance of caesarean section (and the short and long-term complications that accompany this), reduction of delivery time, and general applicability with cephalic presentation (head presentation). Common complications include the possibility of bruising the baby and causing more severe vaginal tears (perineal laceration) than would otherwise be the case. Severe and rare complications (occurring less frequently than 1 in 200) include nerve damage, Descemet's membrane rupture, skull fractures, and cervical cord injury.
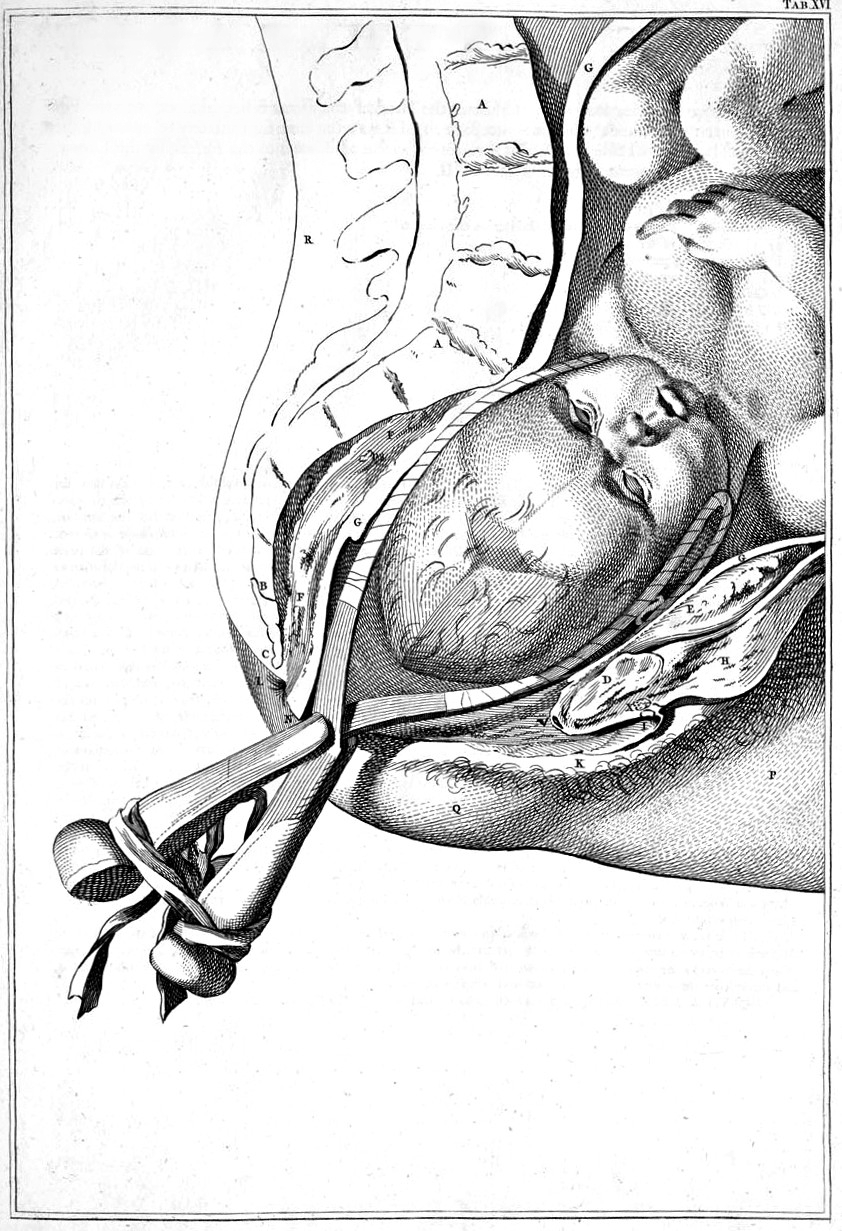
Obstetric forceps consist of two branches (blades) that are positioned around the head of the fetus. These branches are defined as left and right depending on which side of the mother's pelvis they will be applied. The branches usually, but not always, cross at a midpoint, which is called the articulation. Most forceps have a locking mechanism at the articulation, but a few have a sliding mechanism instead that allows the two branches to slide along each other. Forceps with a fixed lock mechanism are used for deliveries where little or no rotation is required, as when the fetal head is in line with the mother's pelvis. Forceps with a sliding lock mechanism are used for deliveries requiring more rotation.[medical citation needed]
The blade of each forceps branch is the curved portion that is used to grasp the fetal head. The forceps should surround the fetal head firmly, but not tightly. The blade characteristically has two curves, the cephalic and the pelvic curves. The cephalic curve is shaped to conform to the fetal head. The cephalic curve can be rounded or rather elongated depending on the shape of the fetal head. The pelvic curve is shaped to conform to the birth canal and helps direct the force of the traction under the pubic bone. Forceps used for rotation of the fetal head should have almost no pelvic curve.[medical citation needed]
The handles are connected to the blades by shanks of variable lengths. Forceps with longer shanks are used if rotation is being considered.[medical citation needed]
All American forceps are derived from French forceps (long forceps) or English forceps (short forceps). Short forceps are applied on the fetal head already descended significantly in the maternal pelvis (i.e., proximal to the vagina). Long forceps are able to reach a fetal head still in the middle or even in the upper part of the maternal pelvis. At present practice, it is uncommon to use forceps to access a fetal head in the upper pelvis. So, short forceps are preferred in the UK and USA. Long forceps are still in use elsewhere.
Simpson forceps (1848) are the most commonly used among the types of forceps and has an elongated cephalic curve. These are used when there is substantial molding, that is, temporary elongation of the fetal head as it moves through the birth canal.[medical citation needed]
Hub AI
Obstetrical forceps AI simulator
(@Obstetrical forceps_simulator)
Obstetrical forceps
Obstetrical forceps are a medical instrument used in childbirth. Their use can serve as an alternative to the ventouse (vacuum extraction) method.
Forceps births, like all assisted births, should be undertaken only to help promote the health of the mother or baby. In general, a forceps birth is likely to be safer for both the mother and baby than the alternatives – either a ventouse birth or a caesarean section – although caveats such as operator skill apply.
Advantages of forceps use include avoidance of caesarean section (and the short and long-term complications that accompany this), reduction of delivery time, and general applicability with cephalic presentation (head presentation). Common complications include the possibility of bruising the baby and causing more severe vaginal tears (perineal laceration) than would otherwise be the case. Severe and rare complications (occurring less frequently than 1 in 200) include nerve damage, Descemet's membrane rupture, skull fractures, and cervical cord injury.
Obstetric forceps consist of two branches (blades) that are positioned around the head of the fetus. These branches are defined as left and right depending on which side of the mother's pelvis they will be applied. The branches usually, but not always, cross at a midpoint, which is called the articulation. Most forceps have a locking mechanism at the articulation, but a few have a sliding mechanism instead that allows the two branches to slide along each other. Forceps with a fixed lock mechanism are used for deliveries where little or no rotation is required, as when the fetal head is in line with the mother's pelvis. Forceps with a sliding lock mechanism are used for deliveries requiring more rotation.[medical citation needed]
The blade of each forceps branch is the curved portion that is used to grasp the fetal head. The forceps should surround the fetal head firmly, but not tightly. The blade characteristically has two curves, the cephalic and the pelvic curves. The cephalic curve is shaped to conform to the fetal head. The cephalic curve can be rounded or rather elongated depending on the shape of the fetal head. The pelvic curve is shaped to conform to the birth canal and helps direct the force of the traction under the pubic bone. Forceps used for rotation of the fetal head should have almost no pelvic curve.[medical citation needed]
The handles are connected to the blades by shanks of variable lengths. Forceps with longer shanks are used if rotation is being considered.[medical citation needed]
All American forceps are derived from French forceps (long forceps) or English forceps (short forceps). Short forceps are applied on the fetal head already descended significantly in the maternal pelvis (i.e., proximal to the vagina). Long forceps are able to reach a fetal head still in the middle or even in the upper part of the maternal pelvis. At present practice, it is uncommon to use forceps to access a fetal head in the upper pelvis. So, short forceps are preferred in the UK and USA. Long forceps are still in use elsewhere.
Simpson forceps (1848) are the most commonly used among the types of forceps and has an elongated cephalic curve. These are used when there is substantial molding, that is, temporary elongation of the fetal head as it moves through the birth canal.[medical citation needed]