
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Haemophilus influenzae AI simulator
(@Haemophilus influenzae_simulator)
Hub AI
Haemophilus influenzae AI simulator
(@Haemophilus influenzae_simulator)
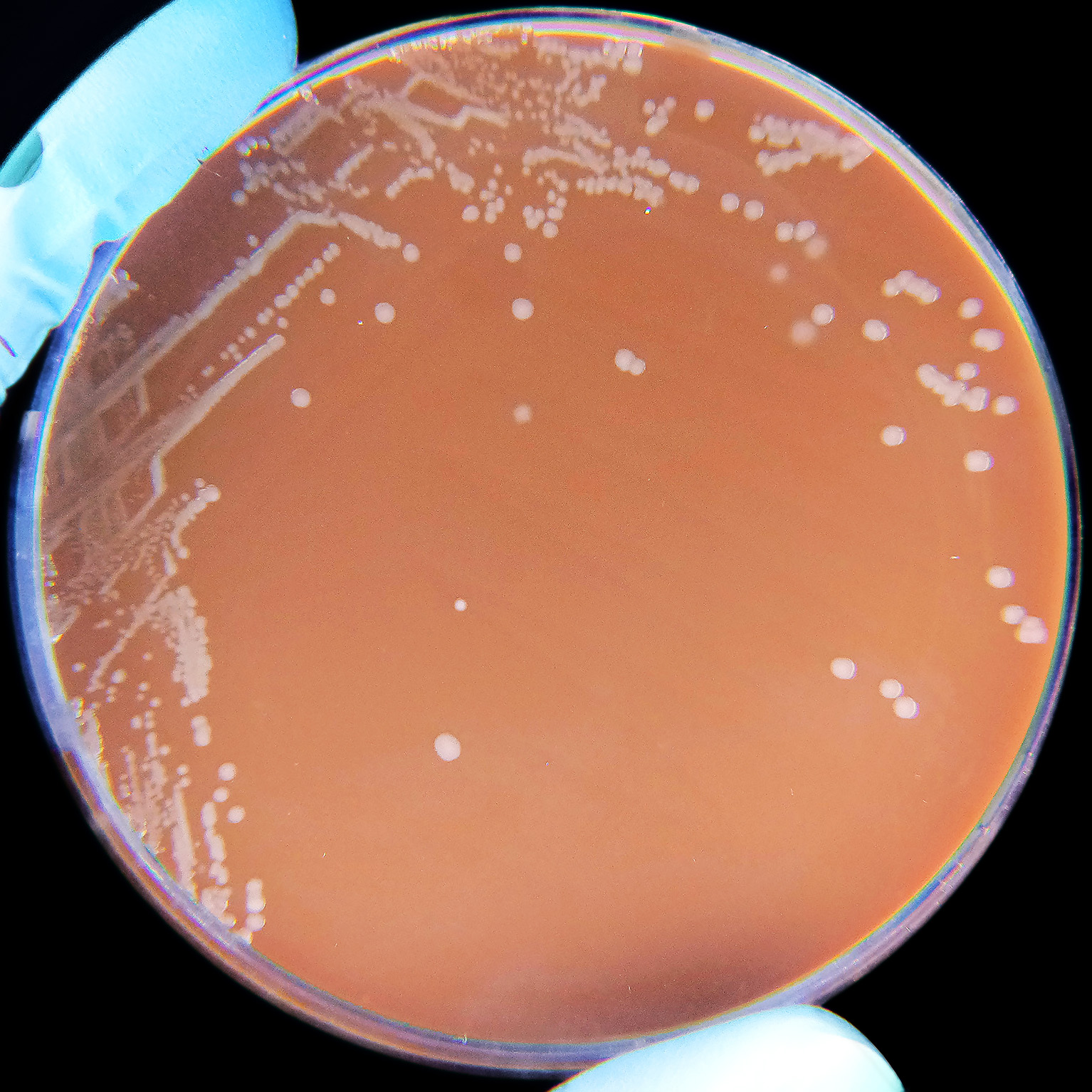
Haemophilus influenzae
Haemophilus influenzae (formerly called Pfeiffer's bacillus or Bacillus influenzae) is a Gram-negative, non-motile, coccobacillary, facultatively anaerobic, capnophilic pathogenic bacterium of the family Pasteurellaceae. The bacteria are mesophilic and grow best at temperatures between 35 and 37 °C.
H. influenzae was first described in 1893 by Richard Pfeiffer during an influenza pandemic when he incorrectly identified it as the causative microbe, which is why the bacteria was given the name "influenzae". H. influenzae is responsible for a wide range of localized and invasive infections, typically in infants and children, including pneumonia, meningitis, or bloodstream infections. Treatment consists of antibiotics; however, H. influenzae is often resistant to the penicillin family, but amoxicillin/clavulanic acid can be used in mild cases. Serotype B H. influenzae (hib) has been a major cause of meningitis in infants and small children, frequently causing deafness and mental degradation. However, the development in the 1980s of a vaccine effective in this age group (the Hib vaccine) has almost eliminated this in developed countries.
This species was the first organism to have its entire genome sequenced.
H. influenzae is a small Gram-negative bacterium, approximately 0.3 micrometer to 1 micrometer. Like other Gram-negative bacteria, H. influenzae has a thin peptidoglycan layer surrounded by an outer membrane containing lipopolysaccharide. Some types of H. influenzae contain a polysaccharide capsule around the outer membrane to aid in protection and colonization. The bacteria are pleomorphic, meaning the shape of the bacterium is variable, however it is typically coccobacillus or rod-shaped. H. Influenzae contains pili, which are specialized to adhere to the human nasopharynx. The H. Influenzae pili, unlike those of E. coli, resist unwinding, allowing for stronger adhesion to resist expulsion when coughing or sneezing. A minority of non-typeable, or unencapsulated, H. influenzae employ a variety of attachment techniques, such as pili, adhesins, or Hia and Hap proteins. Though the bacteria possess pili, they are not used for traditional movement or motility, and the bacterium is still considered to be non-motile.
The cell wall of H. influenzae bacterium contains various proteins, referred to as autotransporters, for adherence and colony formation. H. influenzae prefers to bind to mucus linings or non-ciliated epithelial cells, which is facilitated by Hap𝘴 autotransporters in the cell wall binding with unknown receptors within the epithelium. The Hap𝘴 autotransporters also facilitate the formation of microcolonies of the bacteria. These microcolonies are likely responsible for the formation of various biofilms within the body, such as those responsible for middle ear or lung infections.
Penicillin binding proteins (PBPs) catalyze steps in peptidoglycan metabolism. They carry out essential processes needed to build and modify the cell wall. These proteins are the targets blocked by penicillin and other beta-lactam antibiotics that bind to PBPs, hence their name. Some antibiotic-resistant isolates of H. Influenzae contain modified PBPs that resist beta-lactam action by producing beta-lactamases to degrade these antibiotics. This resistance is likely due to a N526K mutation, or R517H substitution in conjunction with another unknown mutation. The R517H substitution alone did not have a lower affinity for penicillin, and therefore cannot cause resistance alone. Beta-lactamase emergence in the 1970s caused the therapy for severe cases of H. influenzae to be changed from ampicillin to cephalosporins, however further resistance to cephalosporins has occurred due to changes in the transpeptidase domain of penicillin binding protein 3 (PBP3).
H. influenzae isolates were initially characterized as either encapsulated (having an extracellular polysaccharide layer, the bacterial capsule) or unencapsulated. Encapsulated strains were further classified on the basis of the immune response to the type of polysaccharides in their capsule. The six generally recognized types of encapsulated H. influenzae are: a, b, c, d, e, and f. H. Influenzae type b, also known as Hib, is the most common form, recognizable by its polyribosyl ribitol phosphate (PRP) capsule, and found mostly in children. Types a, e, and f have been isolated infrequently, while types d and c are rarely isolated. Unencapsulated strains are more genetically diverse than the encapsulated group. Unencapsulated strains are termed nontypable (NTHi) because they lack capsular serotypes; however, all H. influenzae isolates can now be classified by multilocus sequence typing and other molecular methods. Most NTHi strains are considered to be part of the normal human flora in the upper and lower respiratory tract, genitals, and conjunctivae (mucous membranes of the eye).
H. influenzae uses the Embden–Meyerhof–Parnas (EMP) pathway for glycolysis and the pentose phosphate pathway, which is anabolic rather than catabolic. The citric acid cycle is incomplete and lacks several enzymes that are found in a fully functioning cycle. The enzymes missing from the TCA cycle are citrate synthase, aconitate hydratase, and isocitrate dehydrogenase. H. influenzae has been found in both aerobic and anaerobic environments, as well as environments with different pH's.
Haemophilus influenzae
Haemophilus influenzae (formerly called Pfeiffer's bacillus or Bacillus influenzae) is a Gram-negative, non-motile, coccobacillary, facultatively anaerobic, capnophilic pathogenic bacterium of the family Pasteurellaceae. The bacteria are mesophilic and grow best at temperatures between 35 and 37 °C.
H. influenzae was first described in 1893 by Richard Pfeiffer during an influenza pandemic when he incorrectly identified it as the causative microbe, which is why the bacteria was given the name "influenzae". H. influenzae is responsible for a wide range of localized and invasive infections, typically in infants and children, including pneumonia, meningitis, or bloodstream infections. Treatment consists of antibiotics; however, H. influenzae is often resistant to the penicillin family, but amoxicillin/clavulanic acid can be used in mild cases. Serotype B H. influenzae (hib) has been a major cause of meningitis in infants and small children, frequently causing deafness and mental degradation. However, the development in the 1980s of a vaccine effective in this age group (the Hib vaccine) has almost eliminated this in developed countries.
This species was the first organism to have its entire genome sequenced.
H. influenzae is a small Gram-negative bacterium, approximately 0.3 micrometer to 1 micrometer. Like other Gram-negative bacteria, H. influenzae has a thin peptidoglycan layer surrounded by an outer membrane containing lipopolysaccharide. Some types of H. influenzae contain a polysaccharide capsule around the outer membrane to aid in protection and colonization. The bacteria are pleomorphic, meaning the shape of the bacterium is variable, however it is typically coccobacillus or rod-shaped. H. Influenzae contains pili, which are specialized to adhere to the human nasopharynx. The H. Influenzae pili, unlike those of E. coli, resist unwinding, allowing for stronger adhesion to resist expulsion when coughing or sneezing. A minority of non-typeable, or unencapsulated, H. influenzae employ a variety of attachment techniques, such as pili, adhesins, or Hia and Hap proteins. Though the bacteria possess pili, they are not used for traditional movement or motility, and the bacterium is still considered to be non-motile.
The cell wall of H. influenzae bacterium contains various proteins, referred to as autotransporters, for adherence and colony formation. H. influenzae prefers to bind to mucus linings or non-ciliated epithelial cells, which is facilitated by Hap𝘴 autotransporters in the cell wall binding with unknown receptors within the epithelium. The Hap𝘴 autotransporters also facilitate the formation of microcolonies of the bacteria. These microcolonies are likely responsible for the formation of various biofilms within the body, such as those responsible for middle ear or lung infections.
Penicillin binding proteins (PBPs) catalyze steps in peptidoglycan metabolism. They carry out essential processes needed to build and modify the cell wall. These proteins are the targets blocked by penicillin and other beta-lactam antibiotics that bind to PBPs, hence their name. Some antibiotic-resistant isolates of H. Influenzae contain modified PBPs that resist beta-lactam action by producing beta-lactamases to degrade these antibiotics. This resistance is likely due to a N526K mutation, or R517H substitution in conjunction with another unknown mutation. The R517H substitution alone did not have a lower affinity for penicillin, and therefore cannot cause resistance alone. Beta-lactamase emergence in the 1970s caused the therapy for severe cases of H. influenzae to be changed from ampicillin to cephalosporins, however further resistance to cephalosporins has occurred due to changes in the transpeptidase domain of penicillin binding protein 3 (PBP3).
H. influenzae isolates were initially characterized as either encapsulated (having an extracellular polysaccharide layer, the bacterial capsule) or unencapsulated. Encapsulated strains were further classified on the basis of the immune response to the type of polysaccharides in their capsule. The six generally recognized types of encapsulated H. influenzae are: a, b, c, d, e, and f. H. Influenzae type b, also known as Hib, is the most common form, recognizable by its polyribosyl ribitol phosphate (PRP) capsule, and found mostly in children. Types a, e, and f have been isolated infrequently, while types d and c are rarely isolated. Unencapsulated strains are more genetically diverse than the encapsulated group. Unencapsulated strains are termed nontypable (NTHi) because they lack capsular serotypes; however, all H. influenzae isolates can now be classified by multilocus sequence typing and other molecular methods. Most NTHi strains are considered to be part of the normal human flora in the upper and lower respiratory tract, genitals, and conjunctivae (mucous membranes of the eye).
H. influenzae uses the Embden–Meyerhof–Parnas (EMP) pathway for glycolysis and the pentose phosphate pathway, which is anabolic rather than catabolic. The citric acid cycle is incomplete and lacks several enzymes that are found in a fully functioning cycle. The enzymes missing from the TCA cycle are citrate synthase, aconitate hydratase, and isocitrate dehydrogenase. H. influenzae has been found in both aerobic and anaerobic environments, as well as environments with different pH's.
Recent media
Recent media