Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
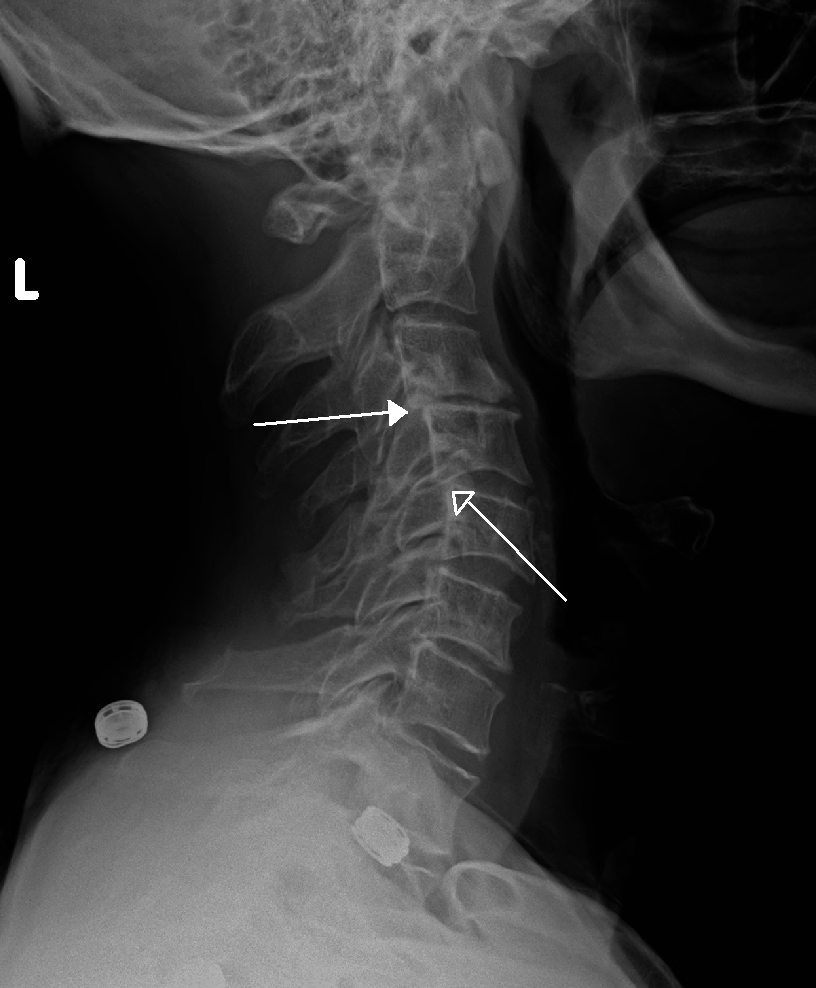
Retrolisthesis
A retrolisthesis is a posterior displacement of one vertebral body with respect to the subjacent vertebra to a degree less than a luxation (dislocation). Retrolistheses are most easily diagnosed on lateral x-ray views of the spine. Views where care has been taken to expose for a true lateral view without any rotation offer the best diagnostic quality.
Retrolistheses are found most prominently in the cervical spine and lumbar region but can also be seen in the thoracic area.
Retrolisthesis can be classified as a form of spondylolisthesis, since spondylolisthesis is often defined in the literature as displacement in any direction. Yet, medical dictionaries usually define spondylolisthesis specifically as the forward or anterior displacement of a vertebra over the vertebra inferior to it (or the sacrum). Retrolisthesis is also called retrospondylolisthesis.
Retrolisthesis may lead to multiple symptoms of greatly varying intensity and distribution. This is because of the variable nature of the impact on nerve tissue and of the mechanical impact on the spinal joints themselves.[citation needed]
Structural instability may be experienced as a local uneasiness through to a more far reaching structural compensatory distortion involving the whole spine. If the joints are stuck in a retrolisthesis configuration there may also be changes to range of motion.[citation needed]
Pain may be experienced as a result of irritation to the sensory nerve roots by bone depending on the degree of displacement and the presence of any rotatory positioning of the individual spinal motion segments. The soft tissue of the disc is often caused to bulge in retrolistheses. These cannot be determined by plain films, as the x-ray passes through the soft tissue. A study by Giles et al., stated that sixteen of the thirty patients (53%) had retrolisthesis of L5 on S1 ranging from 2–9 mm; these patients had either intervertebral disc bulging or protrusion on CT examination ranging from 3–7 mm into the spinal canal. Fourteen patients (47%) without retrolisthesis (control group) did not show any retrolisthesis and the CT did not show any bulge/protrusion. On categorizing x-ray and CT pathology as being present or not, the well positioned i.e. true lateral plain x-ray film revealed a sensitivity and specificity of 100% ([95% Confidence Interval. = [89%–100%]) for bulge/protrusion in this preliminary study.” (7)[citation needed]
Spinal cord compressions are also possible with patients experiencing pain, rigidity and neurologic signs that may follow some distance along nerves to cause symptoms at some distance from the location of the retrolisthesis.[citation needed]
Complete Retrolisthesis - The body of one vertebra is posterior to both the vertebral body of the segment of the spine above as well as below.[citation needed]
Hub AI
Retrolisthesis AI simulator
(@Retrolisthesis_simulator)
Retrolisthesis
A retrolisthesis is a posterior displacement of one vertebral body with respect to the subjacent vertebra to a degree less than a luxation (dislocation). Retrolistheses are most easily diagnosed on lateral x-ray views of the spine. Views where care has been taken to expose for a true lateral view without any rotation offer the best diagnostic quality.
Retrolistheses are found most prominently in the cervical spine and lumbar region but can also be seen in the thoracic area.
Retrolisthesis can be classified as a form of spondylolisthesis, since spondylolisthesis is often defined in the literature as displacement in any direction. Yet, medical dictionaries usually define spondylolisthesis specifically as the forward or anterior displacement of a vertebra over the vertebra inferior to it (or the sacrum). Retrolisthesis is also called retrospondylolisthesis.
Retrolisthesis may lead to multiple symptoms of greatly varying intensity and distribution. This is because of the variable nature of the impact on nerve tissue and of the mechanical impact on the spinal joints themselves.[citation needed]
Structural instability may be experienced as a local uneasiness through to a more far reaching structural compensatory distortion involving the whole spine. If the joints are stuck in a retrolisthesis configuration there may also be changes to range of motion.[citation needed]
Pain may be experienced as a result of irritation to the sensory nerve roots by bone depending on the degree of displacement and the presence of any rotatory positioning of the individual spinal motion segments. The soft tissue of the disc is often caused to bulge in retrolistheses. These cannot be determined by plain films, as the x-ray passes through the soft tissue. A study by Giles et al., stated that sixteen of the thirty patients (53%) had retrolisthesis of L5 on S1 ranging from 2–9 mm; these patients had either intervertebral disc bulging or protrusion on CT examination ranging from 3–7 mm into the spinal canal. Fourteen patients (47%) without retrolisthesis (control group) did not show any retrolisthesis and the CT did not show any bulge/protrusion. On categorizing x-ray and CT pathology as being present or not, the well positioned i.e. true lateral plain x-ray film revealed a sensitivity and specificity of 100% ([95% Confidence Interval. = [89%–100%]) for bulge/protrusion in this preliminary study.” (7)[citation needed]
Spinal cord compressions are also possible with patients experiencing pain, rigidity and neurologic signs that may follow some distance along nerves to cause symptoms at some distance from the location of the retrolisthesis.[citation needed]
Complete Retrolisthesis - The body of one vertebra is posterior to both the vertebral body of the segment of the spine above as well as below.[citation needed]