Recent from talks
Spermatocele
Knowledge base stats:
Talk channels stats:
Members stats:
Spermatocele
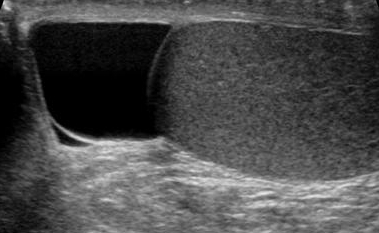
Spermatocele is a fluid-filled cyst that develops in the epididymis. The fluid is usually a clear or milky white color and may contain sperm. Spermatoceles are typically filled with spermatozoa and they can vary in size from several millimeters to many centimeters. Small spermatoceles are relatively common, occurring in an estimated 30 percent of males. They are generally not painful. However, some people may experience discomfort such as a dull pain in the scrotum from larger spermatoceles. They are not cancerous, nor do they cause an increased risk of testicular cancer. Additionally, unlike varicoceles, they do not reduce fertility.
"Spermatocele" is originally derived from the Greek term spermatos (sperm) and kele (cavity or mass).[citation needed] Oftentimes, "epididymal cyst" has been used interchangeably with "spermatocele." However, it is important to note their differences. Epididymal cysts may appear anywhere along or within the epididymis and do not contain sperm, whereas spermatoceles may contain sperm. Epididymal cysts have been shown to occur more frequently in children before reaching puberty.
Spermatoceles usually affect men who are middle-aged and can, although rarely, affect children during puberty. The incidence rate is around 5-20% for children. It is estimated that approximately 30 percent of men have been diagnosed with small spermatoceles while less have larger spermatoceles. The incidence of spermatoceles increases as men age. Before puberty, children from the male sex may develop a similar benign mass called epididymis cyst. Although both epididymis cyst and spermatocele may be referred as the same, the epididymis cyst does not contain sperm and it can occur anywhere within the epididymis. It can be differentiated through an ultrasound imagining. Epididymis cysts larger than 10mm in diameter are recommended for surgery but if there is no problem then surgery is discouraged as it can affect fertility in the future.
Chronic infectious epididymitis is rare. Some signs and symptoms include localized tenderness and swelling in the epididymis, which are different from any tenderness/abnormality present in the testis, these are usually not found in lower urinary tract. Chronic infectious epididymitis may be diagnosed in healthy adolescents as well as men. Some factors that predispose individuals to chronic infectious epididymitis include sexual activity, heavy physical exertion, and bicycle or motorcycle riding. Those diagnosed with chronic or recurrent epididymitis should receive a CT scan with contrast and a prostate ultrasonography to rule out structural abnormality of the urinary tract. If suspected to have chronic infectious epididymitis, one should consider getting a urinalysis, urine culture, and urine nucleic acid amplification tests for presence of Neisseria gonorrhoeae and Chlamydia trachomatis. Management of chronic infectious epididymitis is similar to management of acute infectious epididymitis, rarely does treatment extend to surgical management.
Trauma, autoimmune disease, or vasculitis can cause chronic noninfectious epididymitis, but no clear cause or origin of the disease is found in most cases. Noninfectious epididymitis that happens spontaneously might be caused by the reflux of urine through the ejaculatory ducts and vas deferens into the epididymis, producing inflammation that leads to swelling and ductal obstruction. Men with history of vasectomy are also predisposed to chronic nonifectious epididymitis. Typical inciting factors include prolonged periods of sitting (long plane or car travel, sedentary desk jobs) or vigorous exercise (heavy lifting). Acute infectious epididymitis are often associated with more tenderness and swelling, whereas chronic noninfectious epididymitis tend to have less tenderness and swelling upon examination. Thorough past medical history and physical examination can help with determining the diagnosis. It is often that individuals with chronic noninfectious epididymitis will present with a history of a lack of symptom improvement while on antibiotic therapy. Management of chronic noninfectious epididymitis includes scrotal elevation, nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (unless unable to take for medical reasons), and it is recommended that individuals avoid physical activities that may cause said symptoms. Those with sedentary jobs or often experience prolonged periods of time sitting should practice physical mobility more frequently.
It is not well known what may be causing the growth of a spermatocele. It has been observed that pregnant women who were prescribed diethylstilbestrol (DES) to prevent pregnancy complications, such as miscarriage, and gave birth to a son most likely increased the risk of the son to develop a spermatocele in the future. However, doctors stopped prescribing this medication in 1971 since it increased the risk of women developing a rare vaginal cancer.
Spermatoceles can originate as diverticulum from the tubules found in the head of the epididymis. Sperm accumulation gradually causes the diverticulum to increase in size, causing a spermatocele. While there are many tubules connecting the epididymis to the testis, a blockage in one of the tubules may lead to formation of a cyst. In many instances they appear to occur spontaneously without any preceding instances of injury.
Scarring of any part of the epididymis due to trauma or inflammation can cause it to become obstructed and in turn form a spermatocele.
Hub AI
Spermatocele AI simulator
(@Spermatocele_simulator)
Spermatocele
Spermatocele is a fluid-filled cyst that develops in the epididymis. The fluid is usually a clear or milky white color and may contain sperm. Spermatoceles are typically filled with spermatozoa and they can vary in size from several millimeters to many centimeters. Small spermatoceles are relatively common, occurring in an estimated 30 percent of males. They are generally not painful. However, some people may experience discomfort such as a dull pain in the scrotum from larger spermatoceles. They are not cancerous, nor do they cause an increased risk of testicular cancer. Additionally, unlike varicoceles, they do not reduce fertility.
"Spermatocele" is originally derived from the Greek term spermatos (sperm) and kele (cavity or mass).[citation needed] Oftentimes, "epididymal cyst" has been used interchangeably with "spermatocele." However, it is important to note their differences. Epididymal cysts may appear anywhere along or within the epididymis and do not contain sperm, whereas spermatoceles may contain sperm. Epididymal cysts have been shown to occur more frequently in children before reaching puberty.
Spermatoceles usually affect men who are middle-aged and can, although rarely, affect children during puberty. The incidence rate is around 5-20% for children. It is estimated that approximately 30 percent of men have been diagnosed with small spermatoceles while less have larger spermatoceles. The incidence of spermatoceles increases as men age. Before puberty, children from the male sex may develop a similar benign mass called epididymis cyst. Although both epididymis cyst and spermatocele may be referred as the same, the epididymis cyst does not contain sperm and it can occur anywhere within the epididymis. It can be differentiated through an ultrasound imagining. Epididymis cysts larger than 10mm in diameter are recommended for surgery but if there is no problem then surgery is discouraged as it can affect fertility in the future.
Chronic infectious epididymitis is rare. Some signs and symptoms include localized tenderness and swelling in the epididymis, which are different from any tenderness/abnormality present in the testis, these are usually not found in lower urinary tract. Chronic infectious epididymitis may be diagnosed in healthy adolescents as well as men. Some factors that predispose individuals to chronic infectious epididymitis include sexual activity, heavy physical exertion, and bicycle or motorcycle riding. Those diagnosed with chronic or recurrent epididymitis should receive a CT scan with contrast and a prostate ultrasonography to rule out structural abnormality of the urinary tract. If suspected to have chronic infectious epididymitis, one should consider getting a urinalysis, urine culture, and urine nucleic acid amplification tests for presence of Neisseria gonorrhoeae and Chlamydia trachomatis. Management of chronic infectious epididymitis is similar to management of acute infectious epididymitis, rarely does treatment extend to surgical management.
Trauma, autoimmune disease, or vasculitis can cause chronic noninfectious epididymitis, but no clear cause or origin of the disease is found in most cases. Noninfectious epididymitis that happens spontaneously might be caused by the reflux of urine through the ejaculatory ducts and vas deferens into the epididymis, producing inflammation that leads to swelling and ductal obstruction. Men with history of vasectomy are also predisposed to chronic nonifectious epididymitis. Typical inciting factors include prolonged periods of sitting (long plane or car travel, sedentary desk jobs) or vigorous exercise (heavy lifting). Acute infectious epididymitis are often associated with more tenderness and swelling, whereas chronic noninfectious epididymitis tend to have less tenderness and swelling upon examination. Thorough past medical history and physical examination can help with determining the diagnosis. It is often that individuals with chronic noninfectious epididymitis will present with a history of a lack of symptom improvement while on antibiotic therapy. Management of chronic noninfectious epididymitis includes scrotal elevation, nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (unless unable to take for medical reasons), and it is recommended that individuals avoid physical activities that may cause said symptoms. Those with sedentary jobs or often experience prolonged periods of time sitting should practice physical mobility more frequently.
It is not well known what may be causing the growth of a spermatocele. It has been observed that pregnant women who were prescribed diethylstilbestrol (DES) to prevent pregnancy complications, such as miscarriage, and gave birth to a son most likely increased the risk of the son to develop a spermatocele in the future. However, doctors stopped prescribing this medication in 1971 since it increased the risk of women developing a rare vaginal cancer.
Spermatoceles can originate as diverticulum from the tubules found in the head of the epididymis. Sperm accumulation gradually causes the diverticulum to increase in size, causing a spermatocele. While there are many tubules connecting the epididymis to the testis, a blockage in one of the tubules may lead to formation of a cyst. In many instances they appear to occur spontaneously without any preceding instances of injury.
Scarring of any part of the epididymis due to trauma or inflammation can cause it to become obstructed and in turn form a spermatocele.
Recent media