Recent from talks
Hemothorax
Knowledge base stats:
Talk channels stats:
Members stats:
Hemothorax
A hemothorax (derived from hemo- [blood] + thorax [chest], plural hemothoraces) is an accumulation of blood within the pleural cavity. The symptoms of a hemothorax may include chest pain and difficulty breathing, while the clinical signs may include reduced breath sounds on the affected side and a rapid heart rate. Hemothoraces are usually caused by an injury, but they may occur spontaneously due to cancer invading the pleural cavity, as a result of a blood clotting disorder, as an unusual manifestation of endometriosis, in response to pneumothorax, or rarely in association with other conditions.
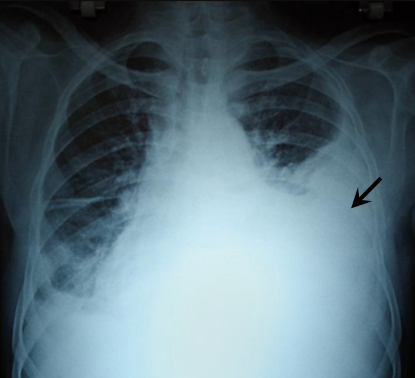
Hemothoraces are usually diagnosed using a chest X-ray, but they can be identified using other forms of imaging including ultrasound, a CT scan, or an MRI. They can be differentiated from other forms of fluid within the pleural cavity by analysing a sample of the fluid, and are defined as having a hematocrit of greater than 50% that of the person's blood. Hemothoraces may be treated by draining the blood using a chest tube. Surgery may be required if the bleeding continues. If treated, the prognosis is usually good. Complications of a hemothorax include infection within the pleural cavity and the formation of scar tissue.
The lungs are surrounded by two layers of tissue called the pulmonary pleurae. In most healthy people, these two layers are tightly apposed, separated only by a small amount of pleural fluid. In certain disease states, the space between these two layers, called the pleural cavity, swells with fluid. This accumulation of fluid in the pleural cavity is called pleural effusion. Pleural effusions are given specific names depending on the nature of the fluid: hydrothorax for serous fluid, pyothorax for pus, hemothorax for blood, and urinothorax for urine.
Signs and symptoms include anxiety, rapid breathing, restlessness, shock, and pale, cool, clammy skin. When the affected area is percussed, a dull feeling may be observed. Neck veins may be flat and breathing sounds reduced. It can also cause a collapsed lung (atelectasis). Massive hemothorax, often defined as over 1.5 liters of blood initially when an intercostal drain is placed, or a bleeding rate greater than 200ml per hour, can result in shock with two causes: massive bleeding resulting from hypovolemic shock, and venous pressure from the retained blood, impairing blood flow.
Hemothoraces are classified in three broad categories according to the cause and in order of frequency: traumatic, iatrogenic, or nontraumatic. All three categories have the potential to affect major arteries and result in death by blood loss.
Hemothorax is most often caused by blunt or penetrating trauma to the chest. In blunt traumatic cases, hemothorax typically occurs when rib fracture damages the intercostal vessels or the intraparenchymal pulmonary vessel, while in penetrating trauma, hemothorax occurs due to injuries directly affecting blood vessels in the thoracic wall, lung parenchyma, or the heart. If large blood vessels such as the aorta are damaged, the blood loss can be massive. Minor chest trauma can cause hemothorax when the blood's ability to clot is diminished as result either of anticoagulant medications or when there are bleeding disorders such as hemophilia.
Iatrogenic hemothorax can occur as a complication of heart and lung surgery, for example the rupture of lung arteries caused by the placement of catheters, thoracotomy, thoracostomy, or thoracentesis. The most common iatrogenic causes include subclavian venous catheterizations and chest tube placements, with an occurrence rate of around 1%. Sometimes, a Swan-Ganz catheter causes rupture of the pulmonary artery, causing a massive hemothorax. It can also be caused by other procedures like pleural, lung, or transbronchial biopsies, CPR, Nuss procedure, or endoscopic treatment of esophageal varices. Iatrogenic hemothorax is more common in people who have chronic kidney disease in the intensive care unit.
Less frequently, hemothoraces may occur spontaneously. Nontraumatic hemothoraces most frequently occur as a complication of some forms of cancer if the tumour invades the pleural space. Cancers responsible for hemothoraces include angiosarcomas, schwannomas, mesothelioma, thymomas, germ cell tumours, and lung cancer. Significant hemothoraces can occur with spontaneous rupture of small vessels when the blood's ability to clot is diminished as result of anticoagulant medications. In cases caused by anticoagulant therapy, the hemothorax becomes noticeable 4–7 days after anticoagulant therapy is started. In cases of hemothorax complicating pulmonary embolism treatment, the hemothorax is usually on the side of the original embolism. Those with an abnormal accumulation of air within the pleural space (a pneumothorax) can bleed into the cavity, which occurs in about 5% of cases of spontaneous pneumothorax, especially when lung bullae rupture. The resulting combination of air and blood within the pleural space is known as a hemopneumothorax. Bone growth in exostosis can create sharp edges, which can result in hemothorax by damaging adjacent arteries. It can occur postpartum due to the change in thoracic pressure during labor.
Hub AI
Hemothorax AI simulator
(@Hemothorax_simulator)
Hemothorax
A hemothorax (derived from hemo- [blood] + thorax [chest], plural hemothoraces) is an accumulation of blood within the pleural cavity. The symptoms of a hemothorax may include chest pain and difficulty breathing, while the clinical signs may include reduced breath sounds on the affected side and a rapid heart rate. Hemothoraces are usually caused by an injury, but they may occur spontaneously due to cancer invading the pleural cavity, as a result of a blood clotting disorder, as an unusual manifestation of endometriosis, in response to pneumothorax, or rarely in association with other conditions.
Hemothoraces are usually diagnosed using a chest X-ray, but they can be identified using other forms of imaging including ultrasound, a CT scan, or an MRI. They can be differentiated from other forms of fluid within the pleural cavity by analysing a sample of the fluid, and are defined as having a hematocrit of greater than 50% that of the person's blood. Hemothoraces may be treated by draining the blood using a chest tube. Surgery may be required if the bleeding continues. If treated, the prognosis is usually good. Complications of a hemothorax include infection within the pleural cavity and the formation of scar tissue.
The lungs are surrounded by two layers of tissue called the pulmonary pleurae. In most healthy people, these two layers are tightly apposed, separated only by a small amount of pleural fluid. In certain disease states, the space between these two layers, called the pleural cavity, swells with fluid. This accumulation of fluid in the pleural cavity is called pleural effusion. Pleural effusions are given specific names depending on the nature of the fluid: hydrothorax for serous fluid, pyothorax for pus, hemothorax for blood, and urinothorax for urine.
Signs and symptoms include anxiety, rapid breathing, restlessness, shock, and pale, cool, clammy skin. When the affected area is percussed, a dull feeling may be observed. Neck veins may be flat and breathing sounds reduced. It can also cause a collapsed lung (atelectasis). Massive hemothorax, often defined as over 1.5 liters of blood initially when an intercostal drain is placed, or a bleeding rate greater than 200ml per hour, can result in shock with two causes: massive bleeding resulting from hypovolemic shock, and venous pressure from the retained blood, impairing blood flow.
Hemothoraces are classified in three broad categories according to the cause and in order of frequency: traumatic, iatrogenic, or nontraumatic. All three categories have the potential to affect major arteries and result in death by blood loss.
Hemothorax is most often caused by blunt or penetrating trauma to the chest. In blunt traumatic cases, hemothorax typically occurs when rib fracture damages the intercostal vessels or the intraparenchymal pulmonary vessel, while in penetrating trauma, hemothorax occurs due to injuries directly affecting blood vessels in the thoracic wall, lung parenchyma, or the heart. If large blood vessels such as the aorta are damaged, the blood loss can be massive. Minor chest trauma can cause hemothorax when the blood's ability to clot is diminished as result either of anticoagulant medications or when there are bleeding disorders such as hemophilia.
Iatrogenic hemothorax can occur as a complication of heart and lung surgery, for example the rupture of lung arteries caused by the placement of catheters, thoracotomy, thoracostomy, or thoracentesis. The most common iatrogenic causes include subclavian venous catheterizations and chest tube placements, with an occurrence rate of around 1%. Sometimes, a Swan-Ganz catheter causes rupture of the pulmonary artery, causing a massive hemothorax. It can also be caused by other procedures like pleural, lung, or transbronchial biopsies, CPR, Nuss procedure, or endoscopic treatment of esophageal varices. Iatrogenic hemothorax is more common in people who have chronic kidney disease in the intensive care unit.
Less frequently, hemothoraces may occur spontaneously. Nontraumatic hemothoraces most frequently occur as a complication of some forms of cancer if the tumour invades the pleural space. Cancers responsible for hemothoraces include angiosarcomas, schwannomas, mesothelioma, thymomas, germ cell tumours, and lung cancer. Significant hemothoraces can occur with spontaneous rupture of small vessels when the blood's ability to clot is diminished as result of anticoagulant medications. In cases caused by anticoagulant therapy, the hemothorax becomes noticeable 4–7 days after anticoagulant therapy is started. In cases of hemothorax complicating pulmonary embolism treatment, the hemothorax is usually on the side of the original embolism. Those with an abnormal accumulation of air within the pleural space (a pneumothorax) can bleed into the cavity, which occurs in about 5% of cases of spontaneous pneumothorax, especially when lung bullae rupture. The resulting combination of air and blood within the pleural space is known as a hemopneumothorax. Bone growth in exostosis can create sharp edges, which can result in hemothorax by damaging adjacent arteries. It can occur postpartum due to the change in thoracic pressure during labor.
Recent media