
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Fibrothorax AI simulator
(@Fibrothorax_simulator)
Hub AI
Fibrothorax AI simulator
(@Fibrothorax_simulator)
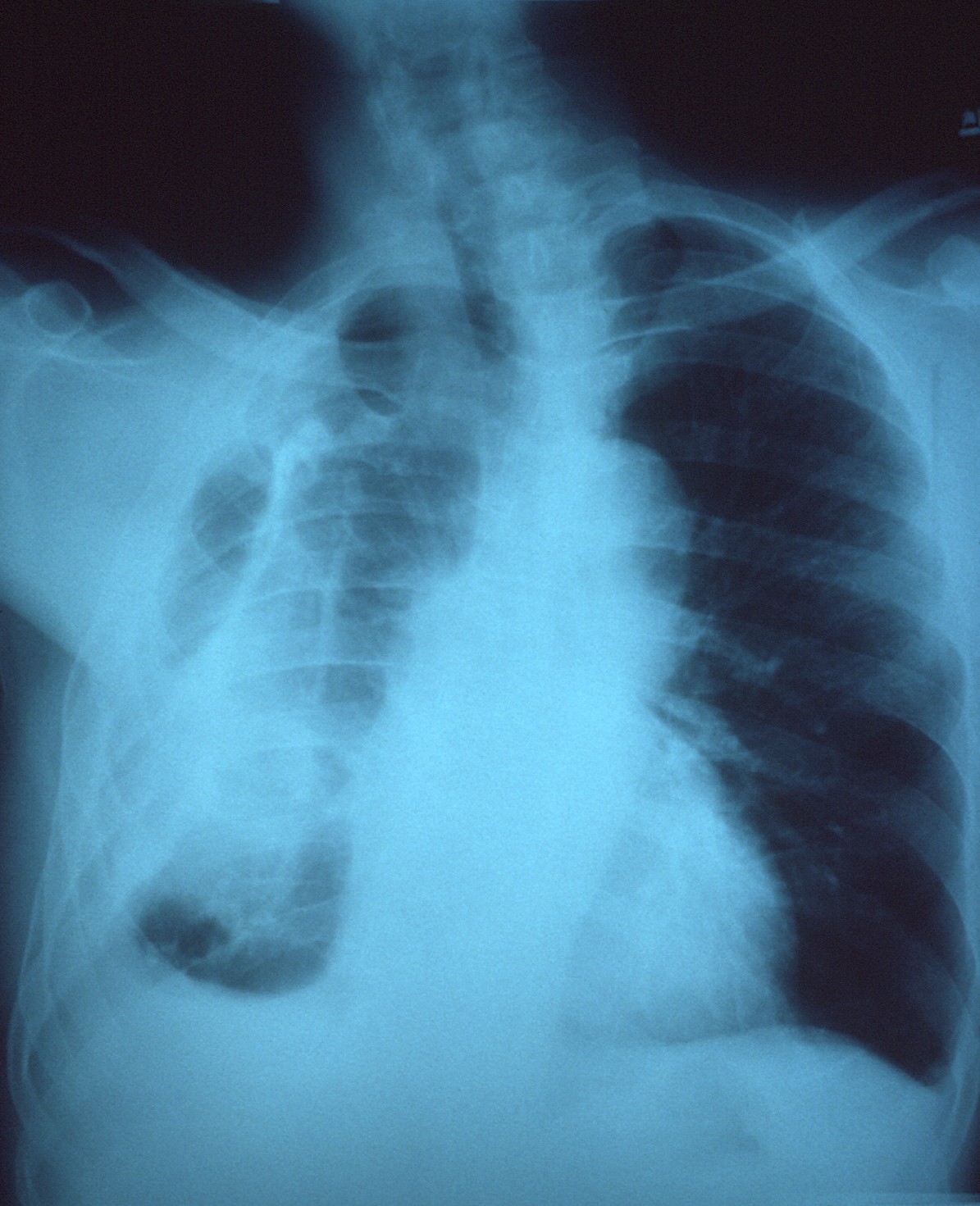
Fibrothorax
Fibrothorax is a medical condition characterised by severe scarring (fibrosis) and fusion of the layers of the pleural space surrounding the lungs resulting in decreased movement of the lung and ribcage. The main symptom of fibrothorax is shortness of breath. There also may be recurrent fluid collections surrounding the lungs. Fibrothorax may occur as a complication of many diseases, including infection of the pleural space known as an empyema or bleeding into the pleural space known as a haemothorax.
Fibrosis in the pleura may be produced intentionally using a technique called pleurodesis to prevent recurrent punctured lung (pneumothorax), and the usually limited fibrosis that this produces can rarely be extensive enough to lead to fibrothorax. The condition is most often diagnosed using an X-ray or CT scan, the latter more readily detecting mild cases. Fibrothorax is often treated conservatively with watchful waiting but may require surgery. The outlook is usually good as long as there is no underlying pulmonary fibrosis or complications following surgery. The disease is highly uncommon.
Reduced movement of the ribcage during breathing, reduced breath sounds on the affected side(s), and a dull feeling when the chest is pressed are common signs observed during examination for fibrothorax. Sharp chest pain with deep breaths or coughing may be seen in some cases. Severe cases of fibrothorax can lead to respiratory failure due to inadequate ventilation and cause abnormally high levels of carbon dioxide in the bloodstream.
The condition only causes symptoms if the visceral pleura is affected. Although fibrothorax may not cause any symptoms, people affected by the disorder may report shortness of breath. Persistent, recurrent pleural effusions are a possible symptom, caused by the persistent cavity formed by the hardening pleura around the original fluid collection. Shortness of breath tends to develop gradually and may worsen over time. Less commonly, fibrothorax may cause chest discomfort or a dry cough. Fibrothorax may occur as a complication of other diseases. Symptoms of the underlying problem are sometimes seen, for example, fever in cases of empyema.
Fibrothorax is often a complication of other diseases that cause inflammation of the pleura. These include infections such as an empyema or tuberculosis, or bleeding within the pleural space known as a haemothorax. Exposure to certain substances, such as asbestos, can cause generalised fibrosis of the lungs, which may involve the pleura and lead to fibrothorax. Less common causes of fibrothorax include collagen vascular diseases such as systemic lupus erythematosus, sarcoidosis, and rheumatoid arthritis; kidney failure leading to uraemia; and side effects of certain medications. The medications most commonly associated with pleural fibrosis are the ergot alkaloids bromocriptine, pergolide, and methysergide. Fibrothorax may also occur without a clear underlying cause, in which case it is known as idiopathic fibrothorax.
A technique called pleurodesis can be used to intentionally create scar tissue within the pleural space, usually as a treatment for repeated episodes of a punctured lung, known as a pneumothorax, or for pleural effusions caused by cancer. While this procedure usually generates only limited scar tissue, in rare cases a fibrothorax can develop.
Fibrosis can affect one or both of the two layers of tissue forming the pleura—the visceral pleura adjacent to the lung and the parietal pleura adjacent to the ribcage. The term fibrothorax implies severe fibrosis affecting both the visceral and the outer (parietal) pleura, fusing the lung to the chest wall. The condition starts as an undrained pleural effusion. Over time, the undrained pleural effusion causes sustained inflammation of the pleura, which can then lead to deposition of fibrin in the pleura and the development of a fibrotic scar. Eventually, a "peel" that is rich in collagen forms around the fluid collection. From this point, the illness can no longer be treated with thoracentesis, since the fluid will return to the cavity maintained by the peel.
Over time, generally over the years, the fibrotic scar tissue slowly tightens and thickens, contracting the contents of one or both halves of the chest and reducing the mobility of the ribs. The peel can become deeper than 2 cm. Within the chest, the lung is compressed and unable to expand (trapped lung), making it vulnerable to collapse and causing breathlessness. Restrictive lung disease from fibrothorax may occur when pleural fibrosis is so severe that it involves the diaphragm and ribcage and results primarily from decreased rib movement.
Fibrothorax
Fibrothorax is a medical condition characterised by severe scarring (fibrosis) and fusion of the layers of the pleural space surrounding the lungs resulting in decreased movement of the lung and ribcage. The main symptom of fibrothorax is shortness of breath. There also may be recurrent fluid collections surrounding the lungs. Fibrothorax may occur as a complication of many diseases, including infection of the pleural space known as an empyema or bleeding into the pleural space known as a haemothorax.
Fibrosis in the pleura may be produced intentionally using a technique called pleurodesis to prevent recurrent punctured lung (pneumothorax), and the usually limited fibrosis that this produces can rarely be extensive enough to lead to fibrothorax. The condition is most often diagnosed using an X-ray or CT scan, the latter more readily detecting mild cases. Fibrothorax is often treated conservatively with watchful waiting but may require surgery. The outlook is usually good as long as there is no underlying pulmonary fibrosis or complications following surgery. The disease is highly uncommon.
Reduced movement of the ribcage during breathing, reduced breath sounds on the affected side(s), and a dull feeling when the chest is pressed are common signs observed during examination for fibrothorax. Sharp chest pain with deep breaths or coughing may be seen in some cases. Severe cases of fibrothorax can lead to respiratory failure due to inadequate ventilation and cause abnormally high levels of carbon dioxide in the bloodstream.
The condition only causes symptoms if the visceral pleura is affected. Although fibrothorax may not cause any symptoms, people affected by the disorder may report shortness of breath. Persistent, recurrent pleural effusions are a possible symptom, caused by the persistent cavity formed by the hardening pleura around the original fluid collection. Shortness of breath tends to develop gradually and may worsen over time. Less commonly, fibrothorax may cause chest discomfort or a dry cough. Fibrothorax may occur as a complication of other diseases. Symptoms of the underlying problem are sometimes seen, for example, fever in cases of empyema.
Fibrothorax is often a complication of other diseases that cause inflammation of the pleura. These include infections such as an empyema or tuberculosis, or bleeding within the pleural space known as a haemothorax. Exposure to certain substances, such as asbestos, can cause generalised fibrosis of the lungs, which may involve the pleura and lead to fibrothorax. Less common causes of fibrothorax include collagen vascular diseases such as systemic lupus erythematosus, sarcoidosis, and rheumatoid arthritis; kidney failure leading to uraemia; and side effects of certain medications. The medications most commonly associated with pleural fibrosis are the ergot alkaloids bromocriptine, pergolide, and methysergide. Fibrothorax may also occur without a clear underlying cause, in which case it is known as idiopathic fibrothorax.
A technique called pleurodesis can be used to intentionally create scar tissue within the pleural space, usually as a treatment for repeated episodes of a punctured lung, known as a pneumothorax, or for pleural effusions caused by cancer. While this procedure usually generates only limited scar tissue, in rare cases a fibrothorax can develop.
Fibrosis can affect one or both of the two layers of tissue forming the pleura—the visceral pleura adjacent to the lung and the parietal pleura adjacent to the ribcage. The term fibrothorax implies severe fibrosis affecting both the visceral and the outer (parietal) pleura, fusing the lung to the chest wall. The condition starts as an undrained pleural effusion. Over time, the undrained pleural effusion causes sustained inflammation of the pleura, which can then lead to deposition of fibrin in the pleura and the development of a fibrotic scar. Eventually, a "peel" that is rich in collagen forms around the fluid collection. From this point, the illness can no longer be treated with thoracentesis, since the fluid will return to the cavity maintained by the peel.
Over time, generally over the years, the fibrotic scar tissue slowly tightens and thickens, contracting the contents of one or both halves of the chest and reducing the mobility of the ribs. The peel can become deeper than 2 cm. Within the chest, the lung is compressed and unable to expand (trapped lung), making it vulnerable to collapse and causing breathlessness. Restrictive lung disease from fibrothorax may occur when pleural fibrosis is so severe that it involves the diaphragm and ribcage and results primarily from decreased rib movement.
Recent media
Recent media