
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Referred pain AI simulator
(@Referred pain_simulator)
Hub AI
Referred pain AI simulator
(@Referred pain_simulator)
Referred pain
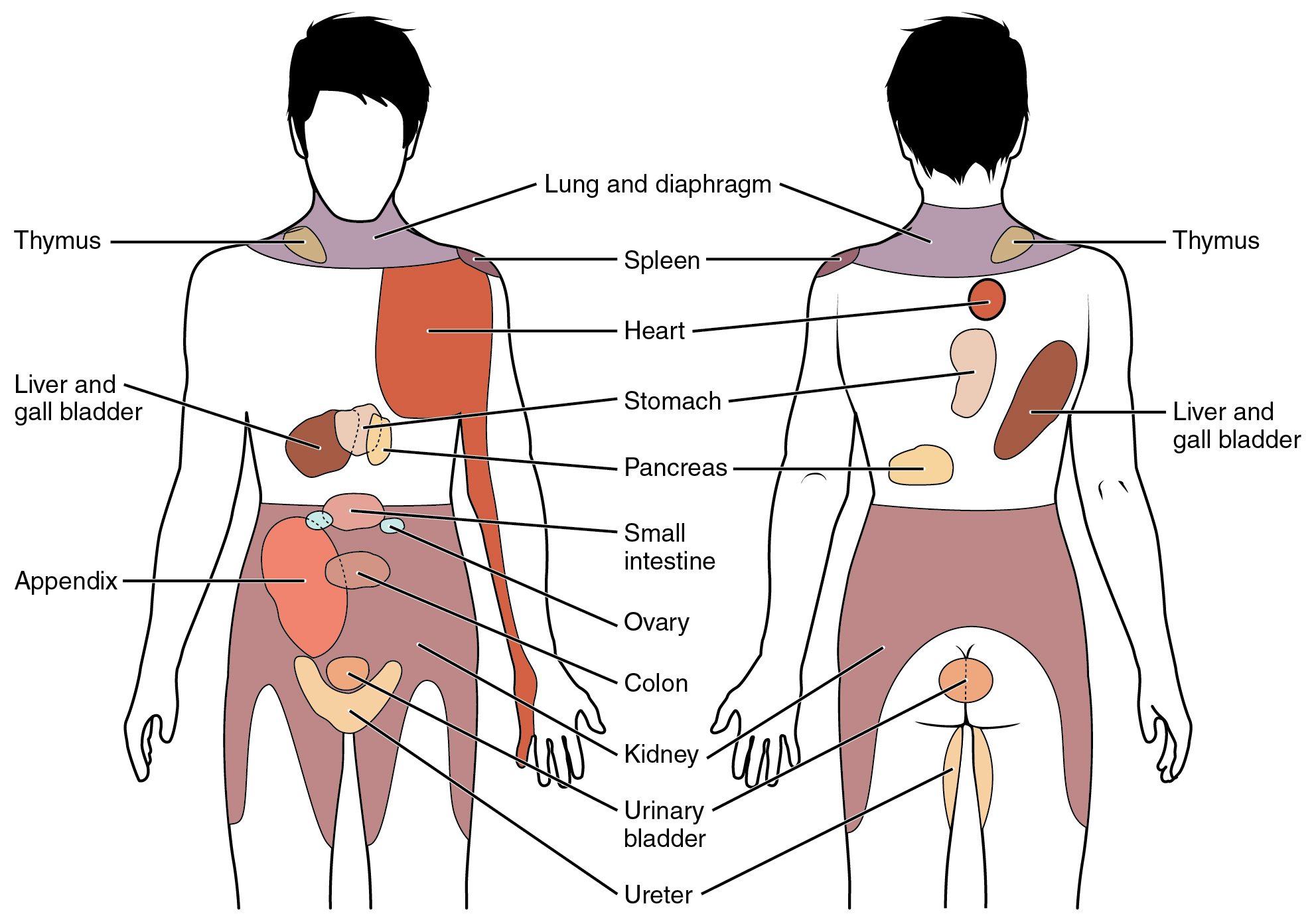
Referred pain, also called reflective pain, is pain perceived at a location other than the site of the painful stimulus. An example is the case of angina pectoris brought on by a myocardial infarction (heart attack), where pain is often felt in the left side of the neck, left shoulder, and back rather than in the thorax (chest), the site of the injury. The International Association for the Study of Pain has not officially defined the term; hence, several authors have defined it differently. Referred pain has been described since the late 1880s. Despite an increasing amount of literature on the subject, the biological mechanism of referred pain is unknown, although there are several hypotheses.
Radiating pain is slightly different from referred pain; for example, the pain related to a myocardial infarction could either be referred or radiating pain from the chest. Referred pain is when the pain is located away from or adjacent to the organ involved; for instance, when a person has pain only in their jaw or left arm, but not in the chest. Radiating pain would have an origin, where the patient can perceive pain, but the pain also spreads ("radiates") out from this origin point to cause the pain to be perceived in a wider area in addition.
There are several proposed mechanisms for referred pain. Currently there is no definitive consensus regarding which is correct. The cardiac general visceral sensory pain fibers follow the sympathetics back to the spinal cord and have their cell bodies located in thoracic dorsal root ganglia 1-4(5). As a general rule, in the thorax and abdomen, general visceral afferent (GVA) pain fibers follow sympathetic fibers back to the same spinal cord segments that gave rise to the preganglionic sympathetic fibers. The central nervous system (CNS) perceives pain from the heart as coming from the somatic portion of the body supplied by the thoracic spinal cord segments 1-4(5). Classically the pain associated with a myocardial infarction is located in the mid or left side of the chest where the heart is actually located. The pain can radiate to the left side of the jaw and into the left arm. Myocardial infarction can rarely present as referred pain and this usually occurs in people with diabetes or older age. Also, the dermatomes of this region of the body wall and upper limb have their neuronal cell bodies in the same dorsal root ganglia (T1-5) and synapse in the same second order neurons in the spinal cord segments (T1-5) as the general visceral sensory fibers from the heart. The CNS does not clearly discern whether the pain is coming from the body wall or from the viscera, but it perceives the pain as coming from somewhere on the body wall, i.e. substernal pain, left arm/hand pain, jaw pain.[citation needed]
This represents one of the earliest theories on the subject of referred pain. It is based on the work of W.A. Sturge and J. Ross from 1888 and later TC Ruch in 1961. Convergent projection proposes that afferent nerve fibers from tissues converge onto the same spinal neuron, and explains why referred pain is believed to be segmented in much the same way as the spinal cord. Additionally, experimental evidence shows that when local pain (pain at the site of stimulation) is intensified the referred pain is intensified as well.[citation needed]
Criticism of this model arises from its inability to explain why there is a delay between the onset of referred pain after local pain stimulation. Experimental evidence also shows that referred pain is often unidirectional. For example, stimulated local pain in the anterior tibial muscle causes referred pain in the ventral portion of the ankle; however referred pain moving in the opposite direction has not been shown experimentally. Lastly, the threshold for the local pain stimulation and the referred pain stimulation are different, but according to this model they should both be the same.
Convergence facilitation was conceived in 1893 by J MacKenzie based on the ideas of Sturge and Ross. He believed that the internal organs were insensitive to stimuli. Furthermore, he believed that non-nociceptive afferent inputs to the spinal cord created what he termed "an irritable focus". This focus caused some stimuli to be perceived as referred pain. However, his ideas did not gain widespread acceptance from critics due to its dismissal of visceral pain.[citation needed]
Recently this idea has regained some credibility under a new term, central sensitization. Central sensitization occurs when neurons in the spinal cord's dorsal horn or brainstem become more responsive after repeated stimulation by peripheral neurons, so that weaker signals can trigger them. The delay in appearance of referred pain shown in laboratory experiments can be explained due to the time required to create the central sensitization.
Axon reflex suggests that the afferent fiber is bifurcated before connecting to the dorsal horn. Bifurcated fibers do exist in muscle, skin, and intervertebral discs. Yet these particular neurons are rare and are not representative of the whole body. Axon-Reflex also does not explain the time delay before the appearance of referred pain, threshold differences for stimulating local and referred pain, and somatosensory sensibility changes in the area of referred pain.
Referred pain
Referred pain, also called reflective pain, is pain perceived at a location other than the site of the painful stimulus. An example is the case of angina pectoris brought on by a myocardial infarction (heart attack), where pain is often felt in the left side of the neck, left shoulder, and back rather than in the thorax (chest), the site of the injury. The International Association for the Study of Pain has not officially defined the term; hence, several authors have defined it differently. Referred pain has been described since the late 1880s. Despite an increasing amount of literature on the subject, the biological mechanism of referred pain is unknown, although there are several hypotheses.
Radiating pain is slightly different from referred pain; for example, the pain related to a myocardial infarction could either be referred or radiating pain from the chest. Referred pain is when the pain is located away from or adjacent to the organ involved; for instance, when a person has pain only in their jaw or left arm, but not in the chest. Radiating pain would have an origin, where the patient can perceive pain, but the pain also spreads ("radiates") out from this origin point to cause the pain to be perceived in a wider area in addition.
There are several proposed mechanisms for referred pain. Currently there is no definitive consensus regarding which is correct. The cardiac general visceral sensory pain fibers follow the sympathetics back to the spinal cord and have their cell bodies located in thoracic dorsal root ganglia 1-4(5). As a general rule, in the thorax and abdomen, general visceral afferent (GVA) pain fibers follow sympathetic fibers back to the same spinal cord segments that gave rise to the preganglionic sympathetic fibers. The central nervous system (CNS) perceives pain from the heart as coming from the somatic portion of the body supplied by the thoracic spinal cord segments 1-4(5). Classically the pain associated with a myocardial infarction is located in the mid or left side of the chest where the heart is actually located. The pain can radiate to the left side of the jaw and into the left arm. Myocardial infarction can rarely present as referred pain and this usually occurs in people with diabetes or older age. Also, the dermatomes of this region of the body wall and upper limb have their neuronal cell bodies in the same dorsal root ganglia (T1-5) and synapse in the same second order neurons in the spinal cord segments (T1-5) as the general visceral sensory fibers from the heart. The CNS does not clearly discern whether the pain is coming from the body wall or from the viscera, but it perceives the pain as coming from somewhere on the body wall, i.e. substernal pain, left arm/hand pain, jaw pain.[citation needed]
This represents one of the earliest theories on the subject of referred pain. It is based on the work of W.A. Sturge and J. Ross from 1888 and later TC Ruch in 1961. Convergent projection proposes that afferent nerve fibers from tissues converge onto the same spinal neuron, and explains why referred pain is believed to be segmented in much the same way as the spinal cord. Additionally, experimental evidence shows that when local pain (pain at the site of stimulation) is intensified the referred pain is intensified as well.[citation needed]
Criticism of this model arises from its inability to explain why there is a delay between the onset of referred pain after local pain stimulation. Experimental evidence also shows that referred pain is often unidirectional. For example, stimulated local pain in the anterior tibial muscle causes referred pain in the ventral portion of the ankle; however referred pain moving in the opposite direction has not been shown experimentally. Lastly, the threshold for the local pain stimulation and the referred pain stimulation are different, but according to this model they should both be the same.
Convergence facilitation was conceived in 1893 by J MacKenzie based on the ideas of Sturge and Ross. He believed that the internal organs were insensitive to stimuli. Furthermore, he believed that non-nociceptive afferent inputs to the spinal cord created what he termed "an irritable focus". This focus caused some stimuli to be perceived as referred pain. However, his ideas did not gain widespread acceptance from critics due to its dismissal of visceral pain.[citation needed]
Recently this idea has regained some credibility under a new term, central sensitization. Central sensitization occurs when neurons in the spinal cord's dorsal horn or brainstem become more responsive after repeated stimulation by peripheral neurons, so that weaker signals can trigger them. The delay in appearance of referred pain shown in laboratory experiments can be explained due to the time required to create the central sensitization.
Axon reflex suggests that the afferent fiber is bifurcated before connecting to the dorsal horn. Bifurcated fibers do exist in muscle, skin, and intervertebral discs. Yet these particular neurons are rare and are not representative of the whole body. Axon-Reflex also does not explain the time delay before the appearance of referred pain, threshold differences for stimulating local and referred pain, and somatosensory sensibility changes in the area of referred pain.
Recent media
Recent media