Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Vascular surgery
Vascular surgery is a surgical subspecialty in which vascular diseases involving the arteries, veins, or lymphatic vessels, are managed by medical therapy, minimally-invasive catheter procedures and surgical reconstruction. The specialty evolved from general and cardiovascular surgery where it refined the management of just the vessels, no longer treating the heart or other organs. Modern vascular surgery includes open surgery techniques, endovascular (minimally invasive) techniques and medical management of vascular diseases – unlike the parent specialities. The vascular surgeon is trained in the diagnosis and management of diseases affecting all parts of the vascular system excluding the coronaries and intracranial vasculature. Vascular surgeons also are called to assist other physicians to carry out surgery near vessels, or to salvage vascular injuries that include hemorrhage control, dissection, occlusion or simply for safe exposure of vascular structures.
Early leaders of the field included Russian surgeon Nikolai Korotkov, noted for developing early surgical techniques, American interventional radiologist Charles Theodore Dotter who is credited with inventing minimally invasive angioplasty (1964), and Australian Robert Paton, who helped the field achieve recognition as a specialty. Edwin Wylie of San Francisco was one of the early American pioneers who developed and fostered advanced training in vascular surgery and pushed for its recognition as a specialty in the United States in the 1970s. The most notable historic figure in vascular surgery is the 1912 Nobel Prize winning surgeon, Alexis Carrel for his techniques used to suture vessels.
The specialty continues to be based on operative arterial and venous surgery but since the early 1990s has evolved greatly. There is now considerable emphasis on minimally invasive alternatives to surgery. The field was originally pioneered by interventional radiologists like Dr. Charles Dotter, who invented angioplasty using serial dilatation of vessels.
The surgeon Dr. Thomas J. Fogarty invented a balloon catheter, designed to remove clots from occluded vessels, which was used as the eventual model to do endovascular angioplasty. Further development of the field has occurred via joint efforts between interventional radiology, vascular surgery, and interventional cardiology. This area of vascular surgery is called Endovascular Surgery or Interventional Vascular Radiology, a term that some in the specialty append to their primary qualification as Vascular Surgeon. Endovascular and endovenous procedures (e.g., EVAR, carotid stenting) can now form the bulk of a vascular surgeon's practice.
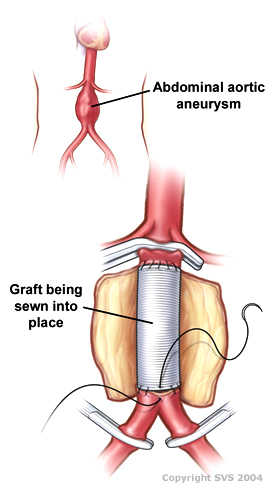
The treatment of the aorta, the body's largest artery, dates back to Greek surgeon Antyllus, who first performed surgeries for various aneurysms in the second century AD. Modern treatment of aortic diseases stems from development and advancements from Michael DeBakey and Denton Cooley. In 1955, DeBakey and Cooley performed the first replacement of a thoracic aneurysm with a homograft. In 1958, they began using the Dacron graft, resulting in a revolution for surgeons in the repair of aortic aneurysms. He also was first to perform cardiopulmonary bypass to repair the ascending aorta, using antegrade perfusion of the brachiocephalic artery.
Dr. Ted Diethrich, one of Dr. DeBakey's associates, went on to pioneer many of the minimally invasive techniques that later became hallmarks of endovascular surgery. Dietrich later founded the Arizona Heart Hospital in 1998 and served as its medical director from 1998 to 2010. In 2000, Diethrich performed the first endovascular aneurysm repair (EVAR) for ruptured abdominal aortic aneurysm. Dietrich trained several future leaders in the field of endovascular surgery at the Arizona Heart Hospital including Venkatesh Ramaiah, MD who succeeded him as medical director of the institution in 2010.
The development of endovascular surgery has been accompanied by a gradual separation of vascular surgery from its origin in general surgery. Most vascular surgeons would now confine their practice to vascular surgery and, similarly, general surgeons would not be trained or practise the larger vascular surgery operations or most endovascular procedures. More recently, professional vascular surgery societies and their training program have formally separated vascular surgery into a separate specialty with its own training program, meetings and accreditation. Notable societies are Society for Vascular Surgery (SVS), USA; Australia and New Zealand Society of Vascular Surgeons (ANZSVS). Local societies also exist (e.g., New South Wales Vascular and Melbourne Vascular Surgical Association (MVSA)). Larger societies of surgery actively separate and encourage specialty surgical societies under their umbrella (e.g., Royal Australasian College of Surgeons (RACS)).
Arterial and venous disease treatment by angiography, stenting, and non-operative varicose vein treatment sclerotherapy, endovenous laser treatment have largely replaced major surgery in many first world countries. These procedures provide reasonable outcomes that are comparable to surgery with the advantage of short hospital stay (day or overnight for most cases) with lower morbidity and mortality rates. Historically performed by interventional radiologists, vascular surgeons have become increasingly proficient with endovascular methods. The durability of endovascular arterial procedures is generally good, especially when viewed in the context of their common clinical usage i.e. arterial disease occurring in elderly patients and usually associated with concurrent significant patient comorbidities especially ischemic heart disease. The cost savings from shorter hospital stays and less morbidity are considerable but are somewhat balanced by the high cost of imaging equipment, construction and staffing of dedicated procedural suites, and of the implant devices themselves. The benefits for younger patients and in venous disease are less persuasive but there are strong trends towards nonoperative treatment options driven by patient preference, health insurance company costs, trial demonstrating comparable efficacy at least in the medium term.
Hub AI
Vascular surgery AI simulator
(@Vascular surgery_simulator)
Vascular surgery
Vascular surgery is a surgical subspecialty in which vascular diseases involving the arteries, veins, or lymphatic vessels, are managed by medical therapy, minimally-invasive catheter procedures and surgical reconstruction. The specialty evolved from general and cardiovascular surgery where it refined the management of just the vessels, no longer treating the heart or other organs. Modern vascular surgery includes open surgery techniques, endovascular (minimally invasive) techniques and medical management of vascular diseases – unlike the parent specialities. The vascular surgeon is trained in the diagnosis and management of diseases affecting all parts of the vascular system excluding the coronaries and intracranial vasculature. Vascular surgeons also are called to assist other physicians to carry out surgery near vessels, or to salvage vascular injuries that include hemorrhage control, dissection, occlusion or simply for safe exposure of vascular structures.
Early leaders of the field included Russian surgeon Nikolai Korotkov, noted for developing early surgical techniques, American interventional radiologist Charles Theodore Dotter who is credited with inventing minimally invasive angioplasty (1964), and Australian Robert Paton, who helped the field achieve recognition as a specialty. Edwin Wylie of San Francisco was one of the early American pioneers who developed and fostered advanced training in vascular surgery and pushed for its recognition as a specialty in the United States in the 1970s. The most notable historic figure in vascular surgery is the 1912 Nobel Prize winning surgeon, Alexis Carrel for his techniques used to suture vessels.
The specialty continues to be based on operative arterial and venous surgery but since the early 1990s has evolved greatly. There is now considerable emphasis on minimally invasive alternatives to surgery. The field was originally pioneered by interventional radiologists like Dr. Charles Dotter, who invented angioplasty using serial dilatation of vessels.
The surgeon Dr. Thomas J. Fogarty invented a balloon catheter, designed to remove clots from occluded vessels, which was used as the eventual model to do endovascular angioplasty. Further development of the field has occurred via joint efforts between interventional radiology, vascular surgery, and interventional cardiology. This area of vascular surgery is called Endovascular Surgery or Interventional Vascular Radiology, a term that some in the specialty append to their primary qualification as Vascular Surgeon. Endovascular and endovenous procedures (e.g., EVAR, carotid stenting) can now form the bulk of a vascular surgeon's practice.
The treatment of the aorta, the body's largest artery, dates back to Greek surgeon Antyllus, who first performed surgeries for various aneurysms in the second century AD. Modern treatment of aortic diseases stems from development and advancements from Michael DeBakey and Denton Cooley. In 1955, DeBakey and Cooley performed the first replacement of a thoracic aneurysm with a homograft. In 1958, they began using the Dacron graft, resulting in a revolution for surgeons in the repair of aortic aneurysms. He also was first to perform cardiopulmonary bypass to repair the ascending aorta, using antegrade perfusion of the brachiocephalic artery.
Dr. Ted Diethrich, one of Dr. DeBakey's associates, went on to pioneer many of the minimally invasive techniques that later became hallmarks of endovascular surgery. Dietrich later founded the Arizona Heart Hospital in 1998 and served as its medical director from 1998 to 2010. In 2000, Diethrich performed the first endovascular aneurysm repair (EVAR) for ruptured abdominal aortic aneurysm. Dietrich trained several future leaders in the field of endovascular surgery at the Arizona Heart Hospital including Venkatesh Ramaiah, MD who succeeded him as medical director of the institution in 2010.
The development of endovascular surgery has been accompanied by a gradual separation of vascular surgery from its origin in general surgery. Most vascular surgeons would now confine their practice to vascular surgery and, similarly, general surgeons would not be trained or practise the larger vascular surgery operations or most endovascular procedures. More recently, professional vascular surgery societies and their training program have formally separated vascular surgery into a separate specialty with its own training program, meetings and accreditation. Notable societies are Society for Vascular Surgery (SVS), USA; Australia and New Zealand Society of Vascular Surgeons (ANZSVS). Local societies also exist (e.g., New South Wales Vascular and Melbourne Vascular Surgical Association (MVSA)). Larger societies of surgery actively separate and encourage specialty surgical societies under their umbrella (e.g., Royal Australasian College of Surgeons (RACS)).
Arterial and venous disease treatment by angiography, stenting, and non-operative varicose vein treatment sclerotherapy, endovenous laser treatment have largely replaced major surgery in many first world countries. These procedures provide reasonable outcomes that are comparable to surgery with the advantage of short hospital stay (day or overnight for most cases) with lower morbidity and mortality rates. Historically performed by interventional radiologists, vascular surgeons have become increasingly proficient with endovascular methods. The durability of endovascular arterial procedures is generally good, especially when viewed in the context of their common clinical usage i.e. arterial disease occurring in elderly patients and usually associated with concurrent significant patient comorbidities especially ischemic heart disease. The cost savings from shorter hospital stays and less morbidity are considerable but are somewhat balanced by the high cost of imaging equipment, construction and staffing of dedicated procedural suites, and of the implant devices themselves. The benefits for younger patients and in venous disease are less persuasive but there are strong trends towards nonoperative treatment options driven by patient preference, health insurance company costs, trial demonstrating comparable efficacy at least in the medium term.