
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Anomic aphasia AI simulator
(@Anomic aphasia_simulator)
Hub AI
Anomic aphasia AI simulator
(@Anomic aphasia_simulator)
Anomic aphasia
Anomic aphasia, also known as dysnomia, nominal aphasia, and amnesic aphasia, is a mild, fluent type of aphasia where individuals have word retrieval failures and cannot express the words they want to say (particularly nouns and verbs). By contrast, anomia is a deficit of expressive language, and a symptom of all forms of aphasia, but patients whose primary deficit is word retrieval are diagnosed with anomic aphasia. Individuals with aphasia who display anomia can often describe an object in detail and maybe even use hand gestures to demonstrate how the object is used, but cannot find the appropriate word to name the object. Patients with anomic aphasia have relatively preserved speech fluency, repetition, comprehension, and grammatical speech.
Anomic aphasia, occurring by itself, may be caused by damage to almost anywhere in the left hemisphere and in some cases can be seen in instances of right hemisphere damage. Anomia can be genetic or caused by damage to various parts of the parietal lobe or the temporal lobe of the brain due to traumatic injury, stroke, or a brain tumor. While anomic aphasia is primarily caused by structural lesions, they may also originate in Alzheimer's disease (anomia may be the earliest language deficit in posterior cortical atrophy variant of Alzheimer's) or other neurodegenerative diseases.
Although the main causes are not specifically known, many researchers have found other factors contributing to anomic aphasia. People with damage to the left hemisphere of the brain are more likely to have anomic aphasia. Broca's area, the speech production center in the brain, was linked to being the source for speech execution problems, with the use of functional magnetic resonance imaging (fMRI), now commonly used to study anomic patients. Other experts believe that damage to Wernicke's area, which is the speech comprehension area of the brain, is connected to anomia because the patients cannot comprehend the words that they are hearing.
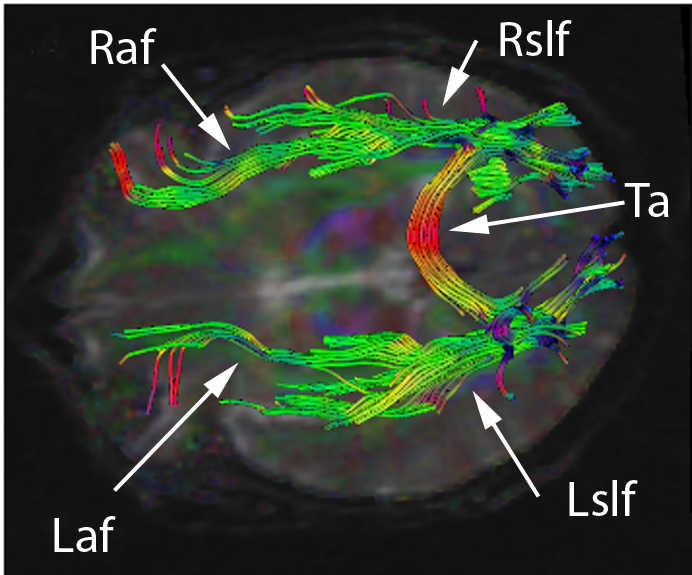
Although many experts have believed that damage to Broca's area or Wernicke's area are the main causes of anomia, current studies have shown that damage in the left parietal lobe is the cause of anomic aphasia. One study was conducted using a word repetition test as well as fMRI in order to see the highest level of activity as well as where the lesions are in the brain tissue. Fridrikkson, et al. saw that damage to neither Broca's area nor Wernicke's area were the sole sources of anomia in the subjects. Therefore, the original anomia model, which theorized that damage occurred on the surface of the brain in the grey matter was debunked, and it was found that the damage was in the white matter deeper in the brain, on the left hemisphere. More specifically, the damage was in a part of the nerve tract called the arcuate fasciculus, for which the mechanism of action is unknown, though it is known to connect the posterior (back) of the brain to the anterior (front) and vice versa.
While anomic aphasia is associated with lesions throughout the left hemisphere, severe and isolated anomia has been considered a sign of deep temporal lobe or lateral temporo-occipital damage. Damage to these areas is seen in patients showing infarction limited to regions supplied by the dominant posterior cerebral artery (PCA) and is referred to as posterior cerebral artery syndrome.
The best way to see if anomic aphasia has developed is by using verbal and imaging tests. The combination seems to be most effective, since either test done alone may give false positives or false negatives. For example, the verbal test is used to see if a speech disorder presents, and whether the problem is in speech production or comprehension. Patients with Alzheimer's disease have speech problems linked to dementia or progressive aphasias, which can include anomia. The imaging test, mostly done using MRI scans, is ideal for lesion mapping or viewing deterioration in the brain. However, imaging cannot diagnose anomia on its own because the lesions may not be located deep enough to damage the white matter or the arcuate fasciculus. However, anomic aphasia is very difficult to associate with a specific lesion location in the brain. Therefore, the combination of speech tests and imaging tests has the highest sensitivity and specificity.
Picture-naming tests, such as the Philadelphia Naming Test (PNT), are also utilized in diagnosing aphasias. Analysis of picture-naming is compared with reading, picture categorizing, and word categorizing. There is a considerable similarity among aphasia syndromes in terms of picture-naming behavior, however anomic aphasiacs produced the fewest phonemic errors and the most multiword circumlocutions. These results suggest minimal word-production difficulty in anomic aphasia relative to other aphasia syndromes.
Anomic aphasia has been diagnosed in some studies using the Aachen Aphasia Test (AAT), which tests language functioning after brain injury. This test aims to: identify the presence of aphasia; provide a profile of the speaker's language functioning according to different language modalities (speaking, listening, reading, writing) and different levels of linguistic description (phonology, morphology, semantics, and syntax); give a measure of severity of any breakdown. This test was administered to patients participating in a study in 2012, and researchers found that on the naming subtest of the AAT patients showed relevant naming difficulties and tended to substitute the words they could not produce with circumlocutions.
Anomic aphasia
Anomic aphasia, also known as dysnomia, nominal aphasia, and amnesic aphasia, is a mild, fluent type of aphasia where individuals have word retrieval failures and cannot express the words they want to say (particularly nouns and verbs). By contrast, anomia is a deficit of expressive language, and a symptom of all forms of aphasia, but patients whose primary deficit is word retrieval are diagnosed with anomic aphasia. Individuals with aphasia who display anomia can often describe an object in detail and maybe even use hand gestures to demonstrate how the object is used, but cannot find the appropriate word to name the object. Patients with anomic aphasia have relatively preserved speech fluency, repetition, comprehension, and grammatical speech.
Anomic aphasia, occurring by itself, may be caused by damage to almost anywhere in the left hemisphere and in some cases can be seen in instances of right hemisphere damage. Anomia can be genetic or caused by damage to various parts of the parietal lobe or the temporal lobe of the brain due to traumatic injury, stroke, or a brain tumor. While anomic aphasia is primarily caused by structural lesions, they may also originate in Alzheimer's disease (anomia may be the earliest language deficit in posterior cortical atrophy variant of Alzheimer's) or other neurodegenerative diseases.
Although the main causes are not specifically known, many researchers have found other factors contributing to anomic aphasia. People with damage to the left hemisphere of the brain are more likely to have anomic aphasia. Broca's area, the speech production center in the brain, was linked to being the source for speech execution problems, with the use of functional magnetic resonance imaging (fMRI), now commonly used to study anomic patients. Other experts believe that damage to Wernicke's area, which is the speech comprehension area of the brain, is connected to anomia because the patients cannot comprehend the words that they are hearing.
Although many experts have believed that damage to Broca's area or Wernicke's area are the main causes of anomia, current studies have shown that damage in the left parietal lobe is the cause of anomic aphasia. One study was conducted using a word repetition test as well as fMRI in order to see the highest level of activity as well as where the lesions are in the brain tissue. Fridrikkson, et al. saw that damage to neither Broca's area nor Wernicke's area were the sole sources of anomia in the subjects. Therefore, the original anomia model, which theorized that damage occurred on the surface of the brain in the grey matter was debunked, and it was found that the damage was in the white matter deeper in the brain, on the left hemisphere. More specifically, the damage was in a part of the nerve tract called the arcuate fasciculus, for which the mechanism of action is unknown, though it is known to connect the posterior (back) of the brain to the anterior (front) and vice versa.
While anomic aphasia is associated with lesions throughout the left hemisphere, severe and isolated anomia has been considered a sign of deep temporal lobe or lateral temporo-occipital damage. Damage to these areas is seen in patients showing infarction limited to regions supplied by the dominant posterior cerebral artery (PCA) and is referred to as posterior cerebral artery syndrome.
The best way to see if anomic aphasia has developed is by using verbal and imaging tests. The combination seems to be most effective, since either test done alone may give false positives or false negatives. For example, the verbal test is used to see if a speech disorder presents, and whether the problem is in speech production or comprehension. Patients with Alzheimer's disease have speech problems linked to dementia or progressive aphasias, which can include anomia. The imaging test, mostly done using MRI scans, is ideal for lesion mapping or viewing deterioration in the brain. However, imaging cannot diagnose anomia on its own because the lesions may not be located deep enough to damage the white matter or the arcuate fasciculus. However, anomic aphasia is very difficult to associate with a specific lesion location in the brain. Therefore, the combination of speech tests and imaging tests has the highest sensitivity and specificity.
Picture-naming tests, such as the Philadelphia Naming Test (PNT), are also utilized in diagnosing aphasias. Analysis of picture-naming is compared with reading, picture categorizing, and word categorizing. There is a considerable similarity among aphasia syndromes in terms of picture-naming behavior, however anomic aphasiacs produced the fewest phonemic errors and the most multiword circumlocutions. These results suggest minimal word-production difficulty in anomic aphasia relative to other aphasia syndromes.
Anomic aphasia has been diagnosed in some studies using the Aachen Aphasia Test (AAT), which tests language functioning after brain injury. This test aims to: identify the presence of aphasia; provide a profile of the speaker's language functioning according to different language modalities (speaking, listening, reading, writing) and different levels of linguistic description (phonology, morphology, semantics, and syntax); give a measure of severity of any breakdown. This test was administered to patients participating in a study in 2012, and researchers found that on the naming subtest of the AAT patients showed relevant naming difficulties and tended to substitute the words they could not produce with circumlocutions.
Recent media
Recent media