Recent from talks
Bone resorption
Knowledge base stats:
Talk channels stats:
Members stats:
Bone resorption
Bone resorption is resorption of bone tissue, that is, the process by which osteoclasts break down the tissue in bones and release the minerals, resulting in a transfer of calcium from bone tissue to the blood.
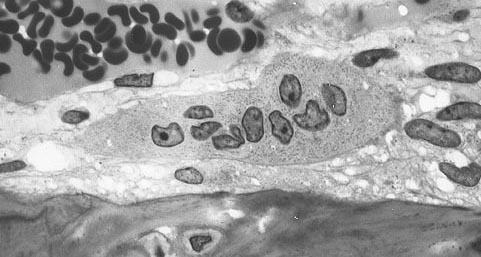
The osteoclasts are multi-nucleated cells that contain numerous mitochondria and lysosomes. These are the cells responsible for the resorption of bone. Osteoblasts are generally present on the outer layer of bone, just beneath the periosteum. Attachment of the osteoclast to the osteon begins the process. The osteoclast then induces an infolding of its cell membrane and secretes collagenase and other enzymes important in the resorption process. High levels of calcium, magnesium, phosphate and products of collagen will be released into the extracellular fluid as the osteoclasts tunnel into the mineralized bone. Osteoclasts are prominent in the tissue destruction found in psoriatic arthritis and rheumatological disorders.
The human body is in a constant state of bone remodeling. Bone remodeling is a process which maintains bone strength and ion homeostasis by replacing discrete parts of old bone with newly synthesized packets of proteinaceous matrix. Bone is resorbed by osteoclasts, and is deposited by osteoblasts in a process called ossification. Osteocyte activity plays a key role in this process. Conditions that result in a decrease in bone mass can either be caused by an increase in resorption or by a decrease in ossification. During childhood, bone formation exceeds resorption. As the aging process occurs, resorption exceeds formation.
Bone resorption rates are much higher in post-menopausal older women due to estrogen deficiency related with menopause. Common treatments include drugs that increase bone mineral density. Bisphosphonates,. RANKL inhibitors, SERMs—selective oestrogen receptor modulators, hormone replacement therapy and calcitonin are some of the common treatments. Light weight-bearing exercise tends to eliminate the negative effects of bone resorption.
Bone resorption is highly stimulated or inhibited by signals from other parts of the body, depending on the demand for calcium.
Calcium-sensing membrane receptors in the parathyroid gland monitor calcium levels in the extracellular fluid. Low levels of calcium stimulates the release of parathyroid hormone (PTH) from chief cells of the parathyroid gland. In addition to its effects on kidney and intestine, PTH increases the number and activity of osteoclasts. The increase in activity of already existing osteoclasts is the initial effect of PTH, and begins in minutes and increases over a few hours. Continued elevation of PTH levels increases the abundance of osteoclasts. This leads to a greater resorption of calcium and phosphate ions.
High levels of calcium in the blood, on the other hand, leads to decreased PTH release from the parathyroid gland, decreasing the number and activity of osteoclasts, resulting in less bone resorption. Vitamin D increases absorption of calcium and phosphate in the intestinal tract, leading to elevated levels of plasma calcium, and thus lower bone resorption.
Calcitriol (1,25-dihydroxycholecalciferol) is the active form of vitamin D3. It has numerous functions involved in blood calcium levels. Recent research indicates that calcitriol leads to a reduction in osteoclast formation, and bone resorption. It follows that an increase in vitamin D3 intake should lead to a decrease in bone resorption — it has been shown that oral administration of vitamin D does not linearly correlate to increased serum levels of calcifediol, the precursor to calcitriol.
Hub AI
Bone resorption AI simulator
(@Bone resorption_simulator)
Bone resorption
Bone resorption is resorption of bone tissue, that is, the process by which osteoclasts break down the tissue in bones and release the minerals, resulting in a transfer of calcium from bone tissue to the blood.
The osteoclasts are multi-nucleated cells that contain numerous mitochondria and lysosomes. These are the cells responsible for the resorption of bone. Osteoblasts are generally present on the outer layer of bone, just beneath the periosteum. Attachment of the osteoclast to the osteon begins the process. The osteoclast then induces an infolding of its cell membrane and secretes collagenase and other enzymes important in the resorption process. High levels of calcium, magnesium, phosphate and products of collagen will be released into the extracellular fluid as the osteoclasts tunnel into the mineralized bone. Osteoclasts are prominent in the tissue destruction found in psoriatic arthritis and rheumatological disorders.
The human body is in a constant state of bone remodeling. Bone remodeling is a process which maintains bone strength and ion homeostasis by replacing discrete parts of old bone with newly synthesized packets of proteinaceous matrix. Bone is resorbed by osteoclasts, and is deposited by osteoblasts in a process called ossification. Osteocyte activity plays a key role in this process. Conditions that result in a decrease in bone mass can either be caused by an increase in resorption or by a decrease in ossification. During childhood, bone formation exceeds resorption. As the aging process occurs, resorption exceeds formation.
Bone resorption rates are much higher in post-menopausal older women due to estrogen deficiency related with menopause. Common treatments include drugs that increase bone mineral density. Bisphosphonates,. RANKL inhibitors, SERMs—selective oestrogen receptor modulators, hormone replacement therapy and calcitonin are some of the common treatments. Light weight-bearing exercise tends to eliminate the negative effects of bone resorption.
Bone resorption is highly stimulated or inhibited by signals from other parts of the body, depending on the demand for calcium.
Calcium-sensing membrane receptors in the parathyroid gland monitor calcium levels in the extracellular fluid. Low levels of calcium stimulates the release of parathyroid hormone (PTH) from chief cells of the parathyroid gland. In addition to its effects on kidney and intestine, PTH increases the number and activity of osteoclasts. The increase in activity of already existing osteoclasts is the initial effect of PTH, and begins in minutes and increases over a few hours. Continued elevation of PTH levels increases the abundance of osteoclasts. This leads to a greater resorption of calcium and phosphate ions.
High levels of calcium in the blood, on the other hand, leads to decreased PTH release from the parathyroid gland, decreasing the number and activity of osteoclasts, resulting in less bone resorption. Vitamin D increases absorption of calcium and phosphate in the intestinal tract, leading to elevated levels of plasma calcium, and thus lower bone resorption.
Calcitriol (1,25-dihydroxycholecalciferol) is the active form of vitamin D3. It has numerous functions involved in blood calcium levels. Recent research indicates that calcitriol leads to a reduction in osteoclast formation, and bone resorption. It follows that an increase in vitamin D3 intake should lead to a decrease in bone resorption — it has been shown that oral administration of vitamin D does not linearly correlate to increased serum levels of calcifediol, the precursor to calcitriol.
Recent media