Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Buttock augmentation
Gluteoplasty (from Greek: gloutós γλουτός, 'rump' + plastos πλαστός, 'shaped, formed, moulded') denotes the plastic surgery and the liposuction procedures for the correction of congenital, traumatic, and acquired defects/deformities of the buttocks and the anatomy of the gluteal region; and for the aesthetic enhancement (by augmentation or by reduction) of the contour of the buttocks.
The procedures for buttock augmentation and buttock repair include the surgical emplacement of a gluteal implant (buttock prosthesis); liposculpture (fat transfer and liposuction); and body contouring (surgery, liposculpture, and Sculptra injections) to resolve the patient's particular concern or deformity of the gluteal region.
The functional purpose of the buttocks musculature is to establish a stable gait (balanced walk) for the person who requires the surgical correction of either a defect or a deformity of the gluteal region; therefore, the restoration of anatomic functionality is the therapeutic consideration that determines which gluteoplasty procedure will effectively correct the damaged muscles of the buttocks. The applicable techniques for surgical and correction include the surgical emplacement of gluteal implants; autologous tissue-flaps; the excision (cutting and removal) of damaged tissues; lipoinjection augmentation; and liposuction reduction—to resolve the defect or deformity caused by a traumatic injury (blunt, penetrating, blast) to the buttocks muscles (gluteus maximus, gluteus medius, gluteus minimus), and any deformation of the anatomic contour of the buttocks. Likewise, the corrective techniques apply to resolving the sagging skin of the body, and the muscle and bone deformities presented by the formerly obese patient, after a massive weight loss (MWL) bariatric surgery procedure; and for resolving congenital defects and congenital deformities of the gluteal region.
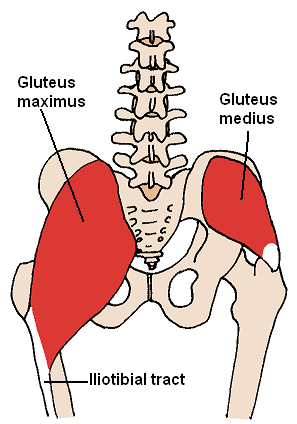
Anatomically, the mass of each buttock principally comprises two muscles—the gluteus maximus muscle and the gluteus medius muscle—which are covered by a layer of adipose body fat. The upper aspects of the buttocks end at the iliac crest (the upper edges of the wings of the ilium, and the upper lateral margins of the greater pelvis), and the lower aspects of the buttocks end at the horizontal gluteal crease, where the buttocks anatomy joins the rear, upper portion of the thighs. The gluteus maximus muscle has two points of insertion: (i) the one-third superior portion of the (coarse line) linea aspera of the thigh bone (femur), and (ii) the superior portion of the iliotibial tract (a long, fibrous reinforcement of the deep fascia lata of the thigh). The left and the right gluteus maximus muscles (the butt cheeks) are vertically divided by the intergluteal cleft (the butt-crack) which contains the anus.
The gluteus maximus muscle is a large and very thick muscle (6–7 cm) located on the sacrum, which is the large, triangular bone located at the base of the vertebral column, and at the upper- and back-part of the pelvic cavity, where it is inserted (like a wedge) between the two hip bones. The upper part of the sacrum is connected to the final lumbar vertebra (L5), and to the bottom of the coccyx (tailbone). At its origin, the gluteus maximus muscle extends to include parts of the iliac bone, the sacrum, the coccyx, the sacrosciatic ligament, and the tuberosity of the ischium.
Like every pelvic-area muscle, the gluteus maximus muscle originates from the pelvis; nonetheless, it is the sole pelvic muscle not inserted to the trochanter (head of the femur), and is approximately aligned to the femur and the fascia lata (the deep fascia of the thigh); the tissues of the gluteus maximus muscle cover only the rear, lateral face of the trochanter, and there form a bursa (purse) that faces the interior of the thigh.
The motor innervation of the gluteus maximus muscle is performed by the inferior gluteal nerve (a branch nerve of the sacral plexus) and extends from the pelvis to the gluteal region, then traverses the greater sciatic foramen (opening) from behind and to the middle to then join the sciatic nerve. The inferior gluteal nerve divides into three collateral branches: (i) the gluteus branch, (ii) the perineal branch, and (iii) the femoral branch. The first ramification—the gluteus branch—is a branch nerve that is very close to the emergence of the inferior gluteal nerve to the area, next to the inferior border of the pyramidalis muscle.
In surgical and body contouring praxis, the plastic surgeon creates the implant-pocket—either for the gluteal prosthesis or for the injections of autologous fat—by undermining the gluteus maximus muscle with a dissection technique that avoids the sacrum, the sacrotuberous ligament, and the tuberosity of the ischium; which, if accidentally cut, might isolate the posterior (back) portion of the muscle and lead to denervation, the loss of nerve function and of innervation.
Hub AI
Buttock augmentation AI simulator
(@Buttock augmentation_simulator)
Buttock augmentation
Gluteoplasty (from Greek: gloutós γλουτός, 'rump' + plastos πλαστός, 'shaped, formed, moulded') denotes the plastic surgery and the liposuction procedures for the correction of congenital, traumatic, and acquired defects/deformities of the buttocks and the anatomy of the gluteal region; and for the aesthetic enhancement (by augmentation or by reduction) of the contour of the buttocks.
The procedures for buttock augmentation and buttock repair include the surgical emplacement of a gluteal implant (buttock prosthesis); liposculpture (fat transfer and liposuction); and body contouring (surgery, liposculpture, and Sculptra injections) to resolve the patient's particular concern or deformity of the gluteal region.
The functional purpose of the buttocks musculature is to establish a stable gait (balanced walk) for the person who requires the surgical correction of either a defect or a deformity of the gluteal region; therefore, the restoration of anatomic functionality is the therapeutic consideration that determines which gluteoplasty procedure will effectively correct the damaged muscles of the buttocks. The applicable techniques for surgical and correction include the surgical emplacement of gluteal implants; autologous tissue-flaps; the excision (cutting and removal) of damaged tissues; lipoinjection augmentation; and liposuction reduction—to resolve the defect or deformity caused by a traumatic injury (blunt, penetrating, blast) to the buttocks muscles (gluteus maximus, gluteus medius, gluteus minimus), and any deformation of the anatomic contour of the buttocks. Likewise, the corrective techniques apply to resolving the sagging skin of the body, and the muscle and bone deformities presented by the formerly obese patient, after a massive weight loss (MWL) bariatric surgery procedure; and for resolving congenital defects and congenital deformities of the gluteal region.
Anatomically, the mass of each buttock principally comprises two muscles—the gluteus maximus muscle and the gluteus medius muscle—which are covered by a layer of adipose body fat. The upper aspects of the buttocks end at the iliac crest (the upper edges of the wings of the ilium, and the upper lateral margins of the greater pelvis), and the lower aspects of the buttocks end at the horizontal gluteal crease, where the buttocks anatomy joins the rear, upper portion of the thighs. The gluteus maximus muscle has two points of insertion: (i) the one-third superior portion of the (coarse line) linea aspera of the thigh bone (femur), and (ii) the superior portion of the iliotibial tract (a long, fibrous reinforcement of the deep fascia lata of the thigh). The left and the right gluteus maximus muscles (the butt cheeks) are vertically divided by the intergluteal cleft (the butt-crack) which contains the anus.
The gluteus maximus muscle is a large and very thick muscle (6–7 cm) located on the sacrum, which is the large, triangular bone located at the base of the vertebral column, and at the upper- and back-part of the pelvic cavity, where it is inserted (like a wedge) between the two hip bones. The upper part of the sacrum is connected to the final lumbar vertebra (L5), and to the bottom of the coccyx (tailbone). At its origin, the gluteus maximus muscle extends to include parts of the iliac bone, the sacrum, the coccyx, the sacrosciatic ligament, and the tuberosity of the ischium.
Like every pelvic-area muscle, the gluteus maximus muscle originates from the pelvis; nonetheless, it is the sole pelvic muscle not inserted to the trochanter (head of the femur), and is approximately aligned to the femur and the fascia lata (the deep fascia of the thigh); the tissues of the gluteus maximus muscle cover only the rear, lateral face of the trochanter, and there form a bursa (purse) that faces the interior of the thigh.
The motor innervation of the gluteus maximus muscle is performed by the inferior gluteal nerve (a branch nerve of the sacral plexus) and extends from the pelvis to the gluteal region, then traverses the greater sciatic foramen (opening) from behind and to the middle to then join the sciatic nerve. The inferior gluteal nerve divides into three collateral branches: (i) the gluteus branch, (ii) the perineal branch, and (iii) the femoral branch. The first ramification—the gluteus branch—is a branch nerve that is very close to the emergence of the inferior gluteal nerve to the area, next to the inferior border of the pyramidalis muscle.
In surgical and body contouring praxis, the plastic surgeon creates the implant-pocket—either for the gluteal prosthesis or for the injections of autologous fat—by undermining the gluteus maximus muscle with a dissection technique that avoids the sacrum, the sacrotuberous ligament, and the tuberosity of the ischium; which, if accidentally cut, might isolate the posterior (back) portion of the muscle and lead to denervation, the loss of nerve function and of innervation.