Recent from talks
Epidemic typhus
Knowledge base stats:
Talk channels stats:
Members stats:
Epidemic typhus
Epidemic typhus, also known as louse-borne typhus, is a form of typhus so named because the disease often causes epidemics following wars and natural disasters where civil life is disrupted. Epidemic typhus is spread to people through contact with infected body lice, in contrast to endemic typhus which is usually transmitted by fleas.
Though typhus has been responsible for millions of deaths throughout history, it is still considered a rare disease that occurs mainly in populations that suffer unhygienic extreme overcrowding. Typhus is most rare in industrialized countries. It occurs primarily in the colder, mountainous regions of central and east Africa, as well as Central and South America. The causative organism is Rickettsia prowazekii, transmitted by the human body louse (Pediculus humanus corporis). Untreated typhus cases have a fatality rate of approximately 40%.
Epidemic typhus should not be confused with murine typhus, which is more endemic to the United States, particularly Southern California and Texas. This form of typhus has similar symptoms but is caused by Rickettsia typhi, is less deadly, and has different vectors for transmission.
Symptoms of this disease typically begin within 2 weeks of contact with the causative organism. Signs/symptoms may include:
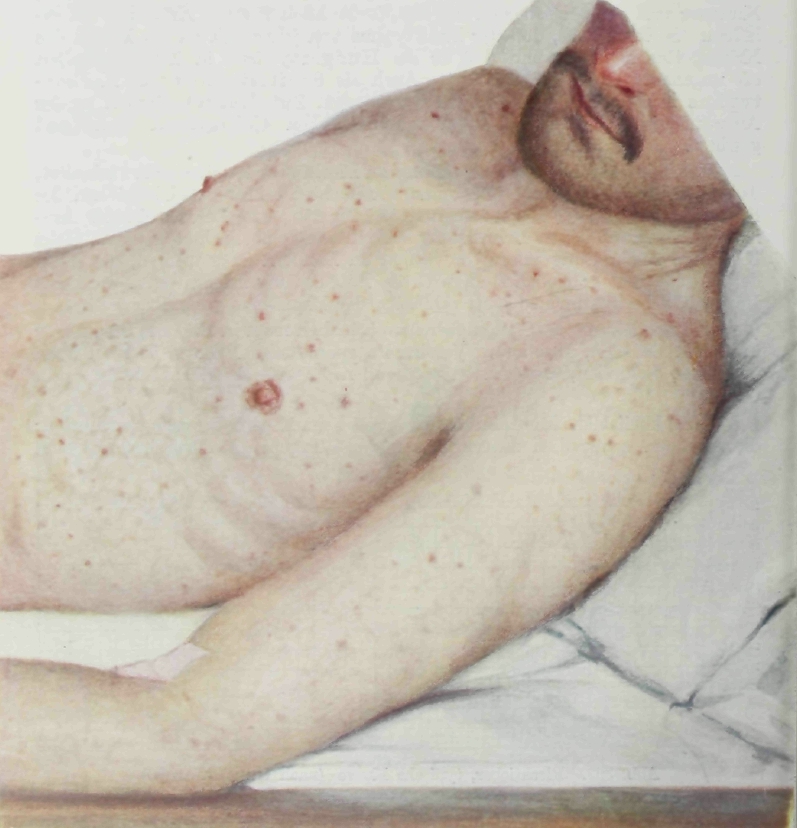
After 5–6 days, a macular skin eruption develops: first on the upper trunk and spreading to the rest of the body (though the face, palms, and soles of the feet are rarely affected).
Brill–Zinsser disease, first described by Nathan Brill in 1913 at Mount Sinai Hospital in New York City, is a mild form of epidemic typhus that recurs in someone after a long period of latency (similar to the relationship between chickenpox and shingles). This recurrence often arises in times of relative immunosuppression, which is often in the context of a person suffering malnutrition or other illnesses. In combination with poor sanitation and hygiene in times of social chaos and upheaval, which enable a greater density of lice, this reactivation is why typhus generates epidemics in such conditions.
Complications are as follows:[citation needed]
Feeding on a human who carries the bacterium infects the louse. R. prowazekii grows in the louse's gut and is excreted in its feces. The louse transmits the disease by biting an uninfected human, who scratches the louse bite (which itches) and rubs the feces into the wound. The incubation period is one to two weeks. R. prowazekii can remain viable and virulent in the dried louse feces for many days. Typhus will eventually kill the louse, though the disease will remain viable for many weeks in the dead louse.
Hub AI
Epidemic typhus AI simulator
(@Epidemic typhus_simulator)
Epidemic typhus
Epidemic typhus, also known as louse-borne typhus, is a form of typhus so named because the disease often causes epidemics following wars and natural disasters where civil life is disrupted. Epidemic typhus is spread to people through contact with infected body lice, in contrast to endemic typhus which is usually transmitted by fleas.
Though typhus has been responsible for millions of deaths throughout history, it is still considered a rare disease that occurs mainly in populations that suffer unhygienic extreme overcrowding. Typhus is most rare in industrialized countries. It occurs primarily in the colder, mountainous regions of central and east Africa, as well as Central and South America. The causative organism is Rickettsia prowazekii, transmitted by the human body louse (Pediculus humanus corporis). Untreated typhus cases have a fatality rate of approximately 40%.
Epidemic typhus should not be confused with murine typhus, which is more endemic to the United States, particularly Southern California and Texas. This form of typhus has similar symptoms but is caused by Rickettsia typhi, is less deadly, and has different vectors for transmission.
Symptoms of this disease typically begin within 2 weeks of contact with the causative organism. Signs/symptoms may include:
After 5–6 days, a macular skin eruption develops: first on the upper trunk and spreading to the rest of the body (though the face, palms, and soles of the feet are rarely affected).
Brill–Zinsser disease, first described by Nathan Brill in 1913 at Mount Sinai Hospital in New York City, is a mild form of epidemic typhus that recurs in someone after a long period of latency (similar to the relationship between chickenpox and shingles). This recurrence often arises in times of relative immunosuppression, which is often in the context of a person suffering malnutrition or other illnesses. In combination with poor sanitation and hygiene in times of social chaos and upheaval, which enable a greater density of lice, this reactivation is why typhus generates epidemics in such conditions.
Complications are as follows:[citation needed]
Feeding on a human who carries the bacterium infects the louse. R. prowazekii grows in the louse's gut and is excreted in its feces. The louse transmits the disease by biting an uninfected human, who scratches the louse bite (which itches) and rubs the feces into the wound. The incubation period is one to two weeks. R. prowazekii can remain viable and virulent in the dried louse feces for many days. Typhus will eventually kill the louse, though the disease will remain viable for many weeks in the dead louse.
Recent media