
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Kwashiorkor AI simulator
(@Kwashiorkor_simulator)
Hub AI
Kwashiorkor AI simulator
(@Kwashiorkor_simulator)
Kwashiorkor
Kwashiorkor (/ˌkwɒʃiˈɔːrkɔːr, -kər/ KWASH-ee-OR-kor, -kər, is a form of severe protein malnutrition characterized by edema and an enlarged liver with fatty infiltrates. It is thought to be caused by sufficient calorie intake, but with insufficient protein consumption (or lack of good quality protein). It is different from marasmus, which is malnutrition of all sources of energy including protein. Recent studies have found that a lack of antioxidant micronutrients such as β-carotene, lycopene, other carotenoids, and vitamin C as well as the presence of aflatoxins may play a role in the development of the disease. However, the exact cause of kwashiorkor is still unknown. Inadequate food supply is correlated with kwashiorkor; occurrences in high-income countries are rare. It occurs amongst weaning children to ages of about five years old.
Conditions analogous to kwashiorkor were well documented around the world throughout history. The disease's first formal description was published by Jamaican pediatrician Cicely Williams in 1933. She was the first to research kwashiorkor, and to suggest that it might be a protein deficiency to differentiate it from other dietary deficiencies.
The name, introduced by Williams in 1935, was derived from the Ga language of coastal Ghana, translated as "the sickness the baby gets when the new baby comes" or "the disease of the deposed child", and reflecting the development of the condition in an older child who has been weaned from the breast when a younger sibling comes. Breast milk contains amino acids vital to a child's growth. In at-risk populations, kwashiorkor is most likely to develop after children are weaned from breast milk and begin consuming a diet high in carbohydrates, including maize, cassava, or rice.
Kwashiorkor is a type of severe acute malnutrition (SAM). SAM is a category, composed of two conditions: marasmus and kwashiorkor. Both kwashiorkor and marasmus fall under the umbrella of protein–energy malnutrition (PEM). These diseases are oftentimes discussed together, but are distinctly separate conditions of malnutrition. Kwashiorkor is marked by an array of metabolic disturbances of uncertain cause. In contrast, marasmus is more clearly an energy deficiency syndrome, marked by weight loss. On physical exam, kwashiorkor is also distinguished from marasmus by the presence of edema. When children present with both kwashiorkor and marasmus, the condition is referred to as "marasmic-kwashiorkor". In general, kwashiorkor is marked by more profound serum depletions of antioxidant molecules and minerals, relative to marasmus.
Wellcome classification is a system for classifying protein-energy malnutrition in children based on weight for their age and based on presence of edema. Other classifications include Gomez classification and Waterlow classification.
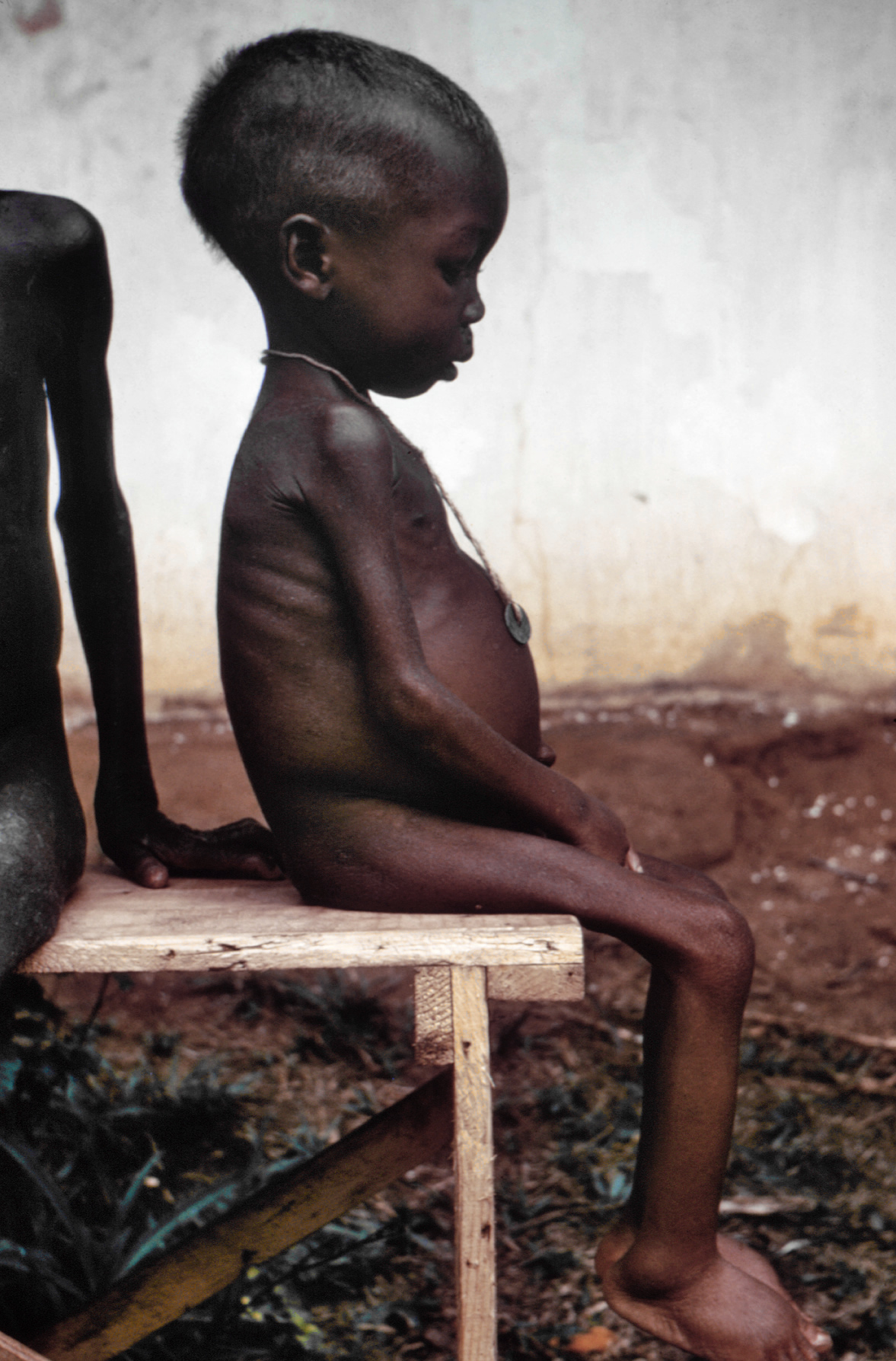
The defining sign of kwashiorkor in children is bilateral edema in the feet. Edema may also involve the hands, trunk, and face. Kwashiorkor is characterized by a fatty liver. This fatty liver of the undernutrition phenotype is often accompanied by evidence of inflammation and fibrosis. Whereas a fatty liver of undernutrition is a consistent feature of kwashiorkor, it is only encountered sometimes in children with marasmus. In addition to this characteristic hepatic steatosis, kwashiorkor is marked by a parallel pattern of multi-organ dysfunction. Organs often affected in children with kwashiorkor include the kidneys, pancreas, heart, and nervous system. Other findings that may be encountered on physical exam include a distended abdomen, hair thinning, loss of teeth, skin or hair depigmentation, and dermatitis. Children with kwashiorkor often develop irritability and anorexia. Generally, kwashiorkor is treated by introducing a high-quality source of protein to the diet. Ready-to-use therapeutic food (RUTF) as well as F-100 and F-75 milk powders, which both include skim milk powder, are recommended for the treatment of kwashiorkor. These products are designed for use in low-resource settings. The limited number of kwashiorkor cases that occur in high resource settings, where there is good access to advanced therapeutic tools, are typically treated with partially hydrolyzed or elemental enteral formulas, with parenteral nutrition provided in extreme cases.
While Kwashiorkor is primarily characterized by edema, growth failure, and dermatitis, it can sometimes be misdiagnosed as Acrodermatitis Enteropathica (AE), as both conditions present with similar dermatological symptoms. However, AE is caused by zinc deficiency, not protein deficiency, and is associated with a significant decrease in serum zinc levels. Unlike kwashiorkor, which is diagnosed based on clinical signs like edema and low serum albumin levels, AE requires additional diagnostic tests, such as zinc uptake tests and genetic screening, to differentiate it from other disorders with similar symptoms. Therefore, while both conditions can present with dermatitis, the underlying etiology helps distinguish the two.
The precise etiology of kwashiorkor remains unclear. Several hypotheses have been proposed that are associated with and explain some, but not all aspects of the pathophysiology of kwashiorkor. They include, but are not limited to protein deficiency causing hypoalbuminemia, amino acid deficiency, oxidative stress, and gut microbiome changes.
Kwashiorkor
Kwashiorkor (/ˌkwɒʃiˈɔːrkɔːr, -kər/ KWASH-ee-OR-kor, -kər, is a form of severe protein malnutrition characterized by edema and an enlarged liver with fatty infiltrates. It is thought to be caused by sufficient calorie intake, but with insufficient protein consumption (or lack of good quality protein). It is different from marasmus, which is malnutrition of all sources of energy including protein. Recent studies have found that a lack of antioxidant micronutrients such as β-carotene, lycopene, other carotenoids, and vitamin C as well as the presence of aflatoxins may play a role in the development of the disease. However, the exact cause of kwashiorkor is still unknown. Inadequate food supply is correlated with kwashiorkor; occurrences in high-income countries are rare. It occurs amongst weaning children to ages of about five years old.
Conditions analogous to kwashiorkor were well documented around the world throughout history. The disease's first formal description was published by Jamaican pediatrician Cicely Williams in 1933. She was the first to research kwashiorkor, and to suggest that it might be a protein deficiency to differentiate it from other dietary deficiencies.
The name, introduced by Williams in 1935, was derived from the Ga language of coastal Ghana, translated as "the sickness the baby gets when the new baby comes" or "the disease of the deposed child", and reflecting the development of the condition in an older child who has been weaned from the breast when a younger sibling comes. Breast milk contains amino acids vital to a child's growth. In at-risk populations, kwashiorkor is most likely to develop after children are weaned from breast milk and begin consuming a diet high in carbohydrates, including maize, cassava, or rice.
Kwashiorkor is a type of severe acute malnutrition (SAM). SAM is a category, composed of two conditions: marasmus and kwashiorkor. Both kwashiorkor and marasmus fall under the umbrella of protein–energy malnutrition (PEM). These diseases are oftentimes discussed together, but are distinctly separate conditions of malnutrition. Kwashiorkor is marked by an array of metabolic disturbances of uncertain cause. In contrast, marasmus is more clearly an energy deficiency syndrome, marked by weight loss. On physical exam, kwashiorkor is also distinguished from marasmus by the presence of edema. When children present with both kwashiorkor and marasmus, the condition is referred to as "marasmic-kwashiorkor". In general, kwashiorkor is marked by more profound serum depletions of antioxidant molecules and minerals, relative to marasmus.
Wellcome classification is a system for classifying protein-energy malnutrition in children based on weight for their age and based on presence of edema. Other classifications include Gomez classification and Waterlow classification.
The defining sign of kwashiorkor in children is bilateral edema in the feet. Edema may also involve the hands, trunk, and face. Kwashiorkor is characterized by a fatty liver. This fatty liver of the undernutrition phenotype is often accompanied by evidence of inflammation and fibrosis. Whereas a fatty liver of undernutrition is a consistent feature of kwashiorkor, it is only encountered sometimes in children with marasmus. In addition to this characteristic hepatic steatosis, kwashiorkor is marked by a parallel pattern of multi-organ dysfunction. Organs often affected in children with kwashiorkor include the kidneys, pancreas, heart, and nervous system. Other findings that may be encountered on physical exam include a distended abdomen, hair thinning, loss of teeth, skin or hair depigmentation, and dermatitis. Children with kwashiorkor often develop irritability and anorexia. Generally, kwashiorkor is treated by introducing a high-quality source of protein to the diet. Ready-to-use therapeutic food (RUTF) as well as F-100 and F-75 milk powders, which both include skim milk powder, are recommended for the treatment of kwashiorkor. These products are designed for use in low-resource settings. The limited number of kwashiorkor cases that occur in high resource settings, where there is good access to advanced therapeutic tools, are typically treated with partially hydrolyzed or elemental enteral formulas, with parenteral nutrition provided in extreme cases.
While Kwashiorkor is primarily characterized by edema, growth failure, and dermatitis, it can sometimes be misdiagnosed as Acrodermatitis Enteropathica (AE), as both conditions present with similar dermatological symptoms. However, AE is caused by zinc deficiency, not protein deficiency, and is associated with a significant decrease in serum zinc levels. Unlike kwashiorkor, which is diagnosed based on clinical signs like edema and low serum albumin levels, AE requires additional diagnostic tests, such as zinc uptake tests and genetic screening, to differentiate it from other disorders with similar symptoms. Therefore, while both conditions can present with dermatitis, the underlying etiology helps distinguish the two.
The precise etiology of kwashiorkor remains unclear. Several hypotheses have been proposed that are associated with and explain some, but not all aspects of the pathophysiology of kwashiorkor. They include, but are not limited to protein deficiency causing hypoalbuminemia, amino acid deficiency, oxidative stress, and gut microbiome changes.
Recent media
Recent media