Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
Multifidus muscle
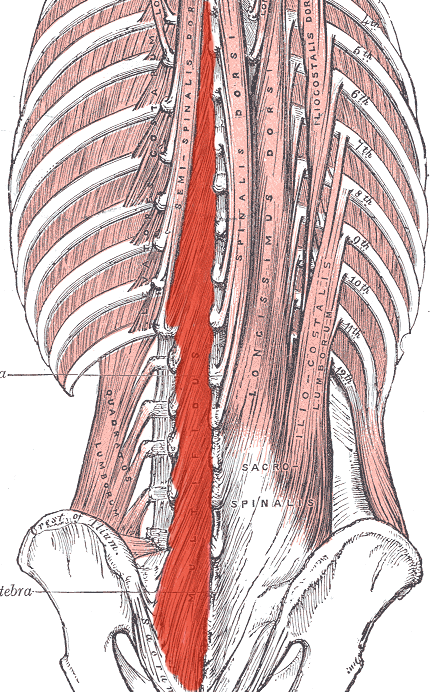
The multifidus (multifidus spinae; pl.: multifidi) muscle consists of a number of fleshy and tendinous fasciculi, which fill up the groove on either side of the spinous processes of the vertebrae, from the sacrum to the axis. While very thin, the multifidus muscle plays an important role in stabilizing the joints within the spine. The multifidus is one of the transversospinales.
Located just superficially to the spine itself, the multifidus muscle spans three joint segments and works to stabilize these joints at each level.
The stiffness and stability makes each vertebra work more effectively, and reduces the degeneration of the joint structures caused by friction from normal physical activity.
These fasciculi arise:
Each fasciculus, passing obliquely upward and medially, is inserted into the whole length of the spinous process of one of the vertebræ above.
These fasciculi vary in length: the most superficial, the longest, pass from one vertebra to the third or fourth above; those next in order run from one vertebra to the second or third above; while the deepest connect two adjacent vertebrae.
The multifidus lies deep relative to the spinal erectors, transverse abdominis, abdominal internal oblique muscle and abdominal external oblique muscle.
Dysfunction in the lumbar multifidus muscles is strongly associated with low back pain. The dysfunction can be caused by inhibition of pain by the spine. The dysfunction frequently persists even after the pain has disappeared. Such persistence may help explain the high recurrence rates of low back pain. Persistent lumbar multifidus dysfunction is diagnosed by atrophic replacement of the multifidus with fat, as visualized by magnetic resonance imaging or ultrasound. One way to help recruit and strengthen the lumbar multifidus muscles is by tensing the pelvic floor muscles for a few seconds "as if stopping urination midstream".
Hub AI
Multifidus muscle AI simulator
(@Multifidus muscle_simulator)
Multifidus muscle
The multifidus (multifidus spinae; pl.: multifidi) muscle consists of a number of fleshy and tendinous fasciculi, which fill up the groove on either side of the spinous processes of the vertebrae, from the sacrum to the axis. While very thin, the multifidus muscle plays an important role in stabilizing the joints within the spine. The multifidus is one of the transversospinales.
Located just superficially to the spine itself, the multifidus muscle spans three joint segments and works to stabilize these joints at each level.
The stiffness and stability makes each vertebra work more effectively, and reduces the degeneration of the joint structures caused by friction from normal physical activity.
These fasciculi arise:
Each fasciculus, passing obliquely upward and medially, is inserted into the whole length of the spinous process of one of the vertebræ above.
These fasciculi vary in length: the most superficial, the longest, pass from one vertebra to the third or fourth above; those next in order run from one vertebra to the second or third above; while the deepest connect two adjacent vertebrae.
The multifidus lies deep relative to the spinal erectors, transverse abdominis, abdominal internal oblique muscle and abdominal external oblique muscle.
Dysfunction in the lumbar multifidus muscles is strongly associated with low back pain. The dysfunction can be caused by inhibition of pain by the spine. The dysfunction frequently persists even after the pain has disappeared. Such persistence may help explain the high recurrence rates of low back pain. Persistent lumbar multifidus dysfunction is diagnosed by atrophic replacement of the multifidus with fat, as visualized by magnetic resonance imaging or ultrasound. One way to help recruit and strengthen the lumbar multifidus muscles is by tensing the pelvic floor muscles for a few seconds "as if stopping urination midstream".