
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Pelvis AI simulator
(@Pelvis_simulator)
Hub AI
Pelvis AI simulator
(@Pelvis_simulator)
Pelvis
The pelvis (pl.: pelves or pelvises) is the lower part of an anatomical trunk, between the abdomen and the thighs (sometimes also called pelvic region), together with its embedded skeleton (sometimes also called bony pelvis or pelvic skeleton).
The pelvic region of the trunk includes the bony pelvis, the pelvic cavity (the space enclosed by the bony pelvis), the pelvic floor, below the pelvic cavity, and the perineum, below the pelvic floor. The pelvic skeleton is formed in the area of the back, by the sacrum and the coccyx and anteriorly and to the left and right sides, by a pair of hip bones.
The two hip bones connect the spine with the lower limbs. They are attached to the sacrum posteriorly, connected to each other anteriorly, and joined with the two femurs at the hip joints. The gap enclosed by the bony pelvis, called the pelvic cavity, is the section of the body underneath the abdomen and mainly consists of the reproductive organs and the rectum, while the pelvic floor at the base of the cavity assists in supporting the organs of the abdomen.
In mammals, the bony pelvis has a gap in the middle, significantly larger in females than in males. Their offspring pass through this gap when they are born.
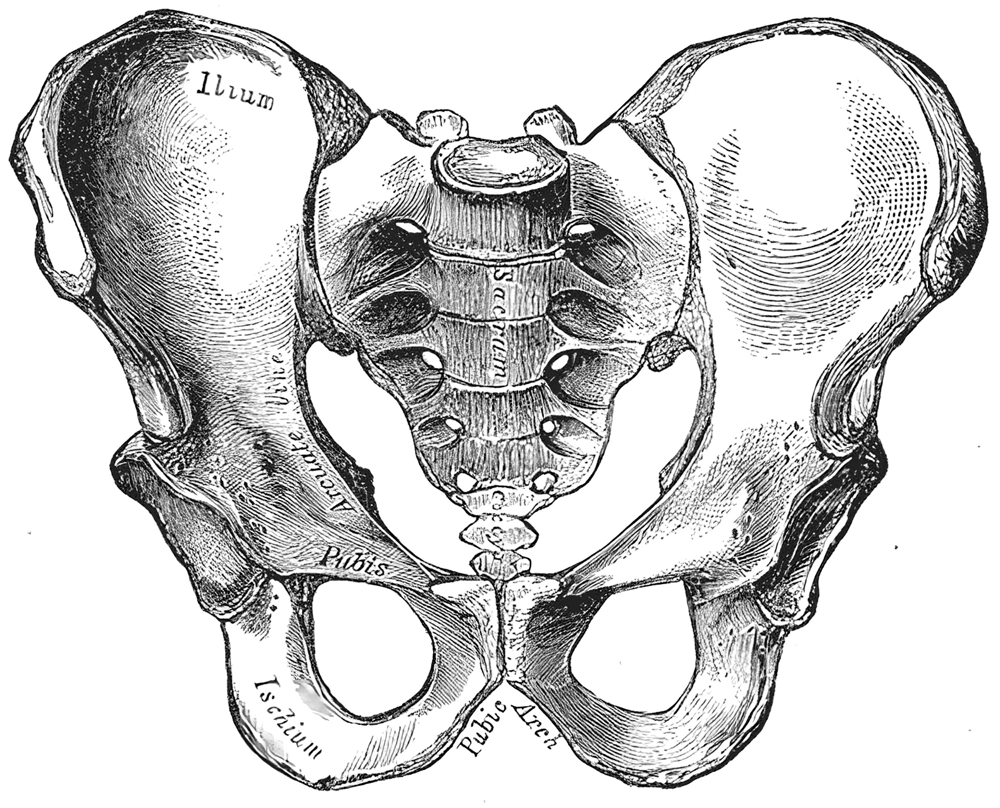
The pelvic region of the trunk is the lower part of the trunk, between the abdomen and the thighs. It includes several structures: the bony pelvis, the pelvic cavity, the pelvic floor, and the perineum. The bony pelvis (pelvic skeleton) is the part of the skeleton embedded in the pelvic region of the trunk. It is subdivided into the pelvic girdle and the pelvic spine. The pelvic girdle is composed of the appendicular hip bones (ilium, ischium, and pubis) oriented in a ring, and connects the pelvic region of the spine to the lower limbs. The pelvic spine consists of the sacrum and coccyx.
The pelvic skeleton is formed posteriorly (in the area of the back), by the sacrum and the coccyx and laterally and anteriorly (forward and to the sides), by a pair of hip bones. Each hip bone consists of three sections: ilium, ischium, and pubis. During childhood, these sections are separate bones, joined by the triradiate cartilage. During puberty, they fuse together to form a single bone.
The pelvic cavity is a body cavity that is bounded by the bones of the pelvis and which primarily contains reproductive organs and the rectum.
A distinction is made between the lesser or true pelvis inferior to the terminal line, and the greater or false pelvis above it. The pelvic inlet or superior pelvic aperture, which leads into the lesser pelvis, is bordered by the promontory, the arcuate line of ilium, the iliopubic eminence, the pecten of the pubis, and the upper part of the pubic symphysis. The pelvic outlet or inferior pelvic aperture is the region between the subpubic angle or pubic arch, the ischial tuberosities and the coccyx.
Pelvis
The pelvis (pl.: pelves or pelvises) is the lower part of an anatomical trunk, between the abdomen and the thighs (sometimes also called pelvic region), together with its embedded skeleton (sometimes also called bony pelvis or pelvic skeleton).
The pelvic region of the trunk includes the bony pelvis, the pelvic cavity (the space enclosed by the bony pelvis), the pelvic floor, below the pelvic cavity, and the perineum, below the pelvic floor. The pelvic skeleton is formed in the area of the back, by the sacrum and the coccyx and anteriorly and to the left and right sides, by a pair of hip bones.
The two hip bones connect the spine with the lower limbs. They are attached to the sacrum posteriorly, connected to each other anteriorly, and joined with the two femurs at the hip joints. The gap enclosed by the bony pelvis, called the pelvic cavity, is the section of the body underneath the abdomen and mainly consists of the reproductive organs and the rectum, while the pelvic floor at the base of the cavity assists in supporting the organs of the abdomen.
In mammals, the bony pelvis has a gap in the middle, significantly larger in females than in males. Their offspring pass through this gap when they are born.
The pelvic region of the trunk is the lower part of the trunk, between the abdomen and the thighs. It includes several structures: the bony pelvis, the pelvic cavity, the pelvic floor, and the perineum. The bony pelvis (pelvic skeleton) is the part of the skeleton embedded in the pelvic region of the trunk. It is subdivided into the pelvic girdle and the pelvic spine. The pelvic girdle is composed of the appendicular hip bones (ilium, ischium, and pubis) oriented in a ring, and connects the pelvic region of the spine to the lower limbs. The pelvic spine consists of the sacrum and coccyx.
The pelvic skeleton is formed posteriorly (in the area of the back), by the sacrum and the coccyx and laterally and anteriorly (forward and to the sides), by a pair of hip bones. Each hip bone consists of three sections: ilium, ischium, and pubis. During childhood, these sections are separate bones, joined by the triradiate cartilage. During puberty, they fuse together to form a single bone.
The pelvic cavity is a body cavity that is bounded by the bones of the pelvis and which primarily contains reproductive organs and the rectum.
A distinction is made between the lesser or true pelvis inferior to the terminal line, and the greater or false pelvis above it. The pelvic inlet or superior pelvic aperture, which leads into the lesser pelvis, is bordered by the promontory, the arcuate line of ilium, the iliopubic eminence, the pecten of the pubis, and the upper part of the pubic symphysis. The pelvic outlet or inferior pelvic aperture is the region between the subpubic angle or pubic arch, the ischial tuberosities and the coccyx.
Recent media
Recent media