Recent from talks
Pulmonary aspiration
Knowledge base stats:
Talk channels stats:
Members stats:
Pulmonary aspiration
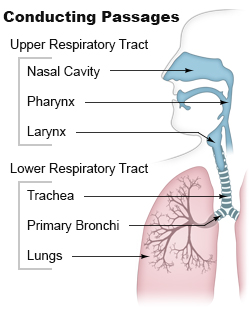
Pulmonary aspiration is the entry of solid or liquid material such as pharyngeal secretions, food, drink, or stomach contents from the oropharynx or gastrointestinal tract, into the trachea and lungs. When pulmonary aspiration occurs during eating and drinking, the aspirated material is often colloquially referred to as "going down the wrong pipe".
Consequences of pulmonary aspiration include no injury at all, chemical pneumonitis, pneumonia, or even death from asphyxiation. These consequences depend on the volume, chemical composition, particle size, and presence of infectious agents in the aspirated material, and on the underlying health status of the person.
In healthy people, aspiration of small quantities of material is common and rarely results in disease or injury. People with significant underlying disease or injury are at greater risk for developing respiratory complications following pulmonary aspiration, especially hospitalized patients, because of certain factors such as depressed level of consciousness and impaired airway defenses (gag reflex and respiratory tract antimicrobial defense system). About 3.6 million cases of pulmonary aspiration or foreign body in the airway occurred in 2013.
Any condition that results in depressed level of consciousness (such as traumatic brain injury, alcohol intoxication, drug overdose, medical sedation, stroke, and general anesthesia) can result in pulmonary aspiration of pharyngeal secretions. Neurologic conditions that affect muscle coordination and posture (such as cerebral palsy, Parkinson's disease, muscular dystrophies, etc.) can also increase risk of aspiration.
Patients with a poor ability to clear their airway of secretions are at an increased risk of pulmonary aspiration. This includes patients with pulmonary disease resulting in a weak cough, or poor forced expiratory volume. Any condition requiring mechanical ventilation is also at risk for aspiration.
Conditions which disrupt coordination of swallowing above the glottis put a patient at increased risk for aspiration. This is referred to as oropharyngeal dysphagia and can be a result of structural abnormalities (strictures, stenosis, mediastinal and neck masses, etc.), connective tissue diseases, neuropathy, or other central nervous system-related disorders (stroke, head injury, ALS, Guillain-Barre, etc.).
Drugs can increase a person's risk of aspiration through multiple mechanisms. Medications including sedatives, hypnotics, and antipsychotics can result in decreased level of consciousness and loss of cough and swallow reflexes. Long-term use of proton pump inhibitors can lead to overgrowth of gastric bacteria and increase risk of aspiration. Antihistamines and antidepressants can cause xerostomia (decreased oral secretions) which can also lead to aspiration.
Particularly common in children, foreign-body aspiration occurs when an object is inhaled from the mouth into the airway. Objects commonly include food, coins, toys and balloons. Age and developmental delays are therefore also considered risk factors for aspiration. The lumen of the right main bronchus is more vertical and slightly wider than that of the left, so aspirated objects are more likely to end up in this bronchus or one of its subsequent bifurcations.
Hub AI
Pulmonary aspiration AI simulator
(@Pulmonary aspiration_simulator)
Pulmonary aspiration
Pulmonary aspiration is the entry of solid or liquid material such as pharyngeal secretions, food, drink, or stomach contents from the oropharynx or gastrointestinal tract, into the trachea and lungs. When pulmonary aspiration occurs during eating and drinking, the aspirated material is often colloquially referred to as "going down the wrong pipe".
Consequences of pulmonary aspiration include no injury at all, chemical pneumonitis, pneumonia, or even death from asphyxiation. These consequences depend on the volume, chemical composition, particle size, and presence of infectious agents in the aspirated material, and on the underlying health status of the person.
In healthy people, aspiration of small quantities of material is common and rarely results in disease or injury. People with significant underlying disease or injury are at greater risk for developing respiratory complications following pulmonary aspiration, especially hospitalized patients, because of certain factors such as depressed level of consciousness and impaired airway defenses (gag reflex and respiratory tract antimicrobial defense system). About 3.6 million cases of pulmonary aspiration or foreign body in the airway occurred in 2013.
Any condition that results in depressed level of consciousness (such as traumatic brain injury, alcohol intoxication, drug overdose, medical sedation, stroke, and general anesthesia) can result in pulmonary aspiration of pharyngeal secretions. Neurologic conditions that affect muscle coordination and posture (such as cerebral palsy, Parkinson's disease, muscular dystrophies, etc.) can also increase risk of aspiration.
Patients with a poor ability to clear their airway of secretions are at an increased risk of pulmonary aspiration. This includes patients with pulmonary disease resulting in a weak cough, or poor forced expiratory volume. Any condition requiring mechanical ventilation is also at risk for aspiration.
Conditions which disrupt coordination of swallowing above the glottis put a patient at increased risk for aspiration. This is referred to as oropharyngeal dysphagia and can be a result of structural abnormalities (strictures, stenosis, mediastinal and neck masses, etc.), connective tissue diseases, neuropathy, or other central nervous system-related disorders (stroke, head injury, ALS, Guillain-Barre, etc.).
Drugs can increase a person's risk of aspiration through multiple mechanisms. Medications including sedatives, hypnotics, and antipsychotics can result in decreased level of consciousness and loss of cough and swallow reflexes. Long-term use of proton pump inhibitors can lead to overgrowth of gastric bacteria and increase risk of aspiration. Antihistamines and antidepressants can cause xerostomia (decreased oral secretions) which can also lead to aspiration.
Particularly common in children, foreign-body aspiration occurs when an object is inhaled from the mouth into the airway. Objects commonly include food, coins, toys and balloons. Age and developmental delays are therefore also considered risk factors for aspiration. The lumen of the right main bronchus is more vertical and slightly wider than that of the left, so aspirated objects are more likely to end up in this bronchus or one of its subsequent bifurcations.
Recent media