

Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Clue cell
View on Wikipedia

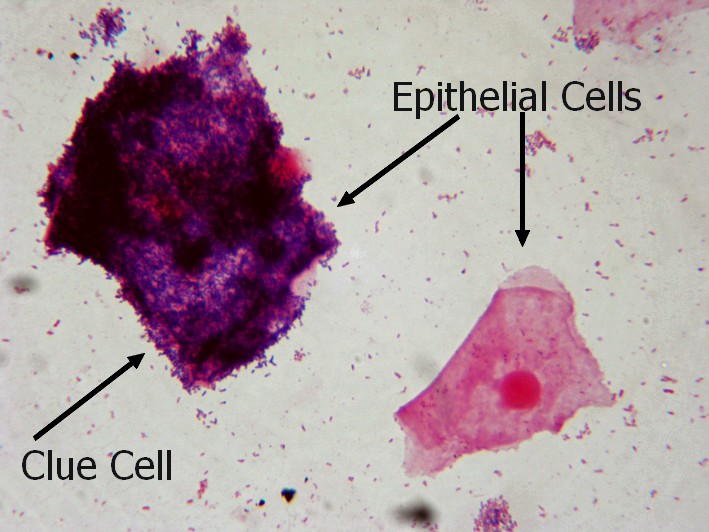
Clue cells are epithelial cells of the vagina that get their distinctive stippled appearance by being covered with bacteria. The etymology behind the term "clue" cell derives from the original research article from Gardner and Dukes describing the characteristic cells. The name was chosen for its brevity in describing the sine qua non of bacterial vaginosis.[1]
They are a medical sign of bacterial vaginosis, particularly that caused by Gardnerella vaginalis,[2] a group of Gram-variable bacteria. This bacterial infection is characterized by thin gray vaginal discharge, and an increase in vaginal pH from around 4.5 to over 5.5.

References
[edit]- ^ Gardner, Herman; Dukes, Charles (May 1955). "Haemophilus vaginalis vaginitis: A newly defined specific infection previously classified "nonspecific" vaginitis". American Journal of Obstetrics and Gynecology. 69 (5): 962–976. doi:10.1016/0002-9378(55)90095-8. PMID 14361525.
- ^ Scott TG, Smyth CJ, Keane CT (February 1987). "In vitro adhesiveness and biotype of Gardnerella vaginalis strains in relation to the occurrence of clue cells in vaginal discharges". Genitourinary Medicine. 63 (1): 47–53. doi:10.1136/sti.63.1.47. PMC 1194007. PMID 3493202.
External links
[edit]- Overview at WebMD
- Clue cell in Gram stain at Fun With Microbiology
- Clue cell in Papanicolaou stain at the http://eknygos.lsmuni.lt/
{kind=link}
{kind=link}
This article related to pathology is a stub. You can help Wikipedia by expanding it. |