
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Compounding AI simulator
(@Compounding_simulator)
Hub AI
Compounding AI simulator
(@Compounding_simulator)
Compounding
In the field of pharmacy, compounding (performed in compounding pharmacies) is preparation of custom medications to fit unique needs of patients that cannot be met with mass-produced formulations. This may be done, for example, to provide medication in a form easier for a given patient to ingest (e.g., liquid vs. tablet), or to avoid a non-active ingredient a patient is allergic to, or to provide an exact dose that isn't otherwise available. This kind of patient-specific compounding, according to a prescriber's specifications, is referred to as "traditional" compounding. The nature of patient need for such customization can range from absolute necessity (e.g. avoiding allergy) to individual optimality (e.g. ideal dose level) to even preference (e.g. flavor or texture).
Hospital pharmacies typically engage in compounding medications for intravenous administration, whereas outpatient or community pharmacies typically engage in compounding medications for oral or topical administration. Due to the rising cost of compounding and drug shortages, some hospitals outsource their compounding needs to large-scale compounding pharmacies, particularly of sterile-injectable medications.
Compounding preparations of a given formulation in advance batches, as opposed to preparation for a specific patient on demand, is known as "non-traditional" compounding and is akin to small-scale manufacturing. Jurisdictions have varying regulations that apply to drug manufacturers and pharmacies that do advance bulk compounding.
The earliest chemists were familiar with various natural substances and their uses. They compounded a variety of preparations such as medications, dyes, incense, perfumes, ceremonial compounds, preservatives and cosmetics. In the medieval Islamic world in particular, Muslim pharmacists and chemists developed advanced methods of compounding drugs. The first drugstores were opened by Muslim pharmacists in Baghdad in 754. The modern age of pharmacy compounding began in the 19th century with the isolation of various compounds from coal tar for the purpose of producing synthetic dyes. From this came the earliest antibacterial sulfa drugs, phenolic compounds made famous by Joseph Lister, and plastics.
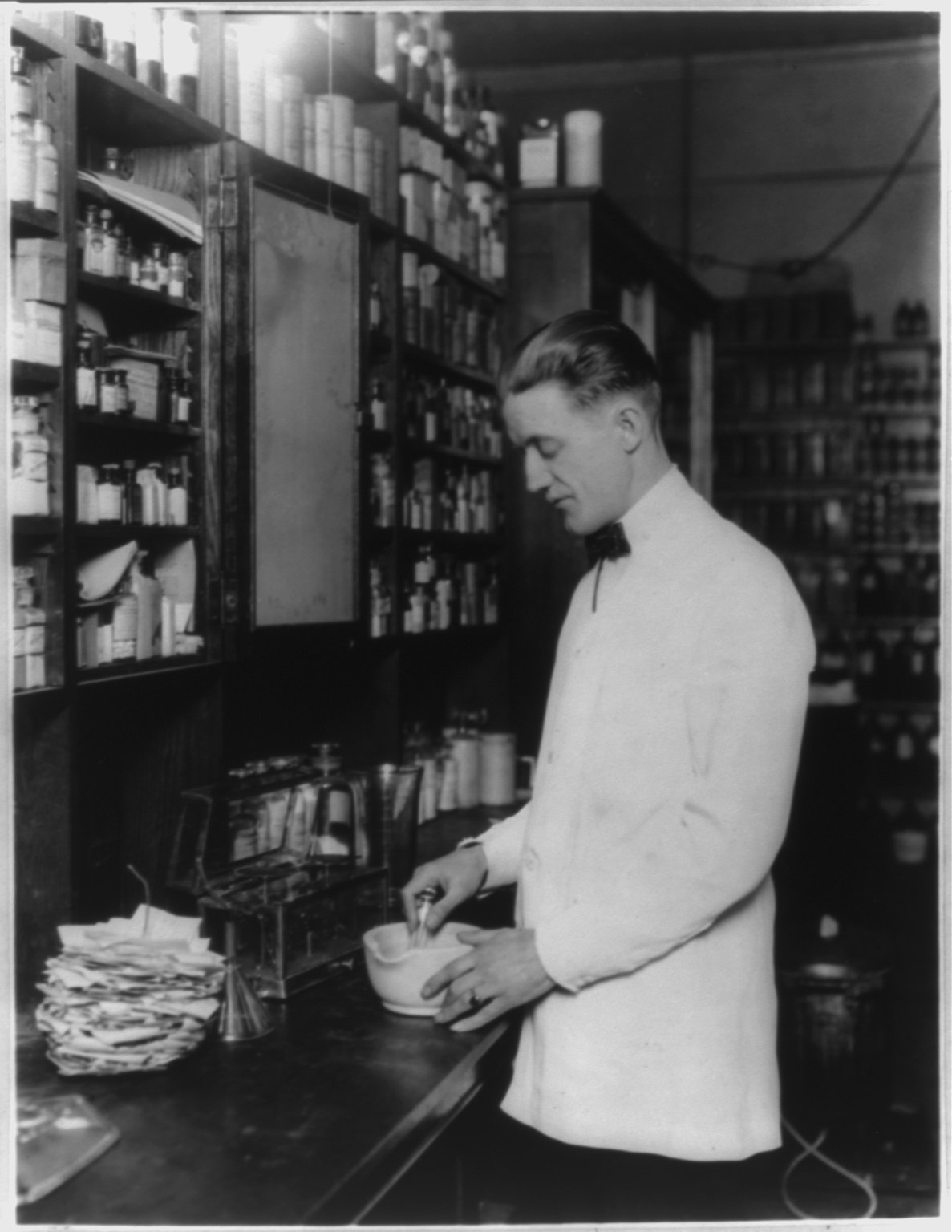
During the 1800s, pharmacists specialized in the raising, preparation and compounding of crude drugs. Crude drugs, like opium, are from natural sources and usually contain several chemical compounds. The pharmacist extracted these drugs using solvents such as water or alcohol to form extracts, concoctions[disambiguation needed] and decoctions. They eventually began isolating and identifying the active ingredients in these drug concoctions. Using fractionation or recrystallization, they separated an active ingredient from the crude preparation, and compounded a medication using this active ingredient.
With the isolation of medications from the raw materials or crude drugs came the birth of the modern pharmaceutical company. Pharmacists were trained to compound the preparations made by the drug companies, but they could not do it efficiently on a small scale. So economies of scale, not lack of skill or knowledge, produced the modern pharmaceutical industry. With the turn of the 20th century came greater government regulation of the practice of medicine. These new regulations forced the drug companies to prove that any new medication they brought to market was safe. With the discovery of penicillin, modern marketing techniques and brand promotion, the drug manufacturing industry came of age. Pharmacists continued to compound most prescriptions until the early 1950s when the majority of dispensed drugs came directly from the large pharmaceutical companies.
A physician may choose to prescribe a compounded medication for a patient with an unusual health need that cannot be met with commercially manufactured products. The physician may choose to prescribe a compounded medication for reasons such as
In hospitals, pharmacists and pharmacy technicians often make compounded sterile preparations (CSPs) using manual methods. The error rate for manually compounded sterile IV products is high. The Institute for Safe Medication Practices (ISMP) has expressed concern with manual methods, particularly the error-prone nature of the syringe pull-back method of verifying sterile preparations. To increase accuracy, some U.S. hospitals have adopted IV workflow management systems and robotic compounding systems. These technologies use barcode scanning to identify each ingredient and gravimetric weight measurement to confirm the proper dose amount. The workflow management systems incorporate software to guide pharmacy technicians through the process of preparing IV medications. The robotic systems prepare IV syringes and bags in an ISO Class 5 environment, and support sterility and dose accuracy by removing human error and contamination from the process.
Compounding
In the field of pharmacy, compounding (performed in compounding pharmacies) is preparation of custom medications to fit unique needs of patients that cannot be met with mass-produced formulations. This may be done, for example, to provide medication in a form easier for a given patient to ingest (e.g., liquid vs. tablet), or to avoid a non-active ingredient a patient is allergic to, or to provide an exact dose that isn't otherwise available. This kind of patient-specific compounding, according to a prescriber's specifications, is referred to as "traditional" compounding. The nature of patient need for such customization can range from absolute necessity (e.g. avoiding allergy) to individual optimality (e.g. ideal dose level) to even preference (e.g. flavor or texture).
Hospital pharmacies typically engage in compounding medications for intravenous administration, whereas outpatient or community pharmacies typically engage in compounding medications for oral or topical administration. Due to the rising cost of compounding and drug shortages, some hospitals outsource their compounding needs to large-scale compounding pharmacies, particularly of sterile-injectable medications.
Compounding preparations of a given formulation in advance batches, as opposed to preparation for a specific patient on demand, is known as "non-traditional" compounding and is akin to small-scale manufacturing. Jurisdictions have varying regulations that apply to drug manufacturers and pharmacies that do advance bulk compounding.
The earliest chemists were familiar with various natural substances and their uses. They compounded a variety of preparations such as medications, dyes, incense, perfumes, ceremonial compounds, preservatives and cosmetics. In the medieval Islamic world in particular, Muslim pharmacists and chemists developed advanced methods of compounding drugs. The first drugstores were opened by Muslim pharmacists in Baghdad in 754. The modern age of pharmacy compounding began in the 19th century with the isolation of various compounds from coal tar for the purpose of producing synthetic dyes. From this came the earliest antibacterial sulfa drugs, phenolic compounds made famous by Joseph Lister, and plastics.
During the 1800s, pharmacists specialized in the raising, preparation and compounding of crude drugs. Crude drugs, like opium, are from natural sources and usually contain several chemical compounds. The pharmacist extracted these drugs using solvents such as water or alcohol to form extracts, concoctions[disambiguation needed] and decoctions. They eventually began isolating and identifying the active ingredients in these drug concoctions. Using fractionation or recrystallization, they separated an active ingredient from the crude preparation, and compounded a medication using this active ingredient.
With the isolation of medications from the raw materials or crude drugs came the birth of the modern pharmaceutical company. Pharmacists were trained to compound the preparations made by the drug companies, but they could not do it efficiently on a small scale. So economies of scale, not lack of skill or knowledge, produced the modern pharmaceutical industry. With the turn of the 20th century came greater government regulation of the practice of medicine. These new regulations forced the drug companies to prove that any new medication they brought to market was safe. With the discovery of penicillin, modern marketing techniques and brand promotion, the drug manufacturing industry came of age. Pharmacists continued to compound most prescriptions until the early 1950s when the majority of dispensed drugs came directly from the large pharmaceutical companies.
A physician may choose to prescribe a compounded medication for a patient with an unusual health need that cannot be met with commercially manufactured products. The physician may choose to prescribe a compounded medication for reasons such as
In hospitals, pharmacists and pharmacy technicians often make compounded sterile preparations (CSPs) using manual methods. The error rate for manually compounded sterile IV products is high. The Institute for Safe Medication Practices (ISMP) has expressed concern with manual methods, particularly the error-prone nature of the syringe pull-back method of verifying sterile preparations. To increase accuracy, some U.S. hospitals have adopted IV workflow management systems and robotic compounding systems. These technologies use barcode scanning to identify each ingredient and gravimetric weight measurement to confirm the proper dose amount. The workflow management systems incorporate software to guide pharmacy technicians through the process of preparing IV medications. The robotic systems prepare IV syringes and bags in an ISO Class 5 environment, and support sterility and dose accuracy by removing human error and contamination from the process.
Recent media
Recent media