Recent from talks
Metabolic acidosis
Knowledge base stats:
Talk channels stats:
Members stats:
Metabolic acidosis
Metabolic acidosis is a serious electrolyte disorder characterized by an imbalance in the body's acid-base balance. Metabolic acidosis has three main root causes: increased acid production, loss of bicarbonate, and a reduced ability of the kidneys to excrete excess acids. Metabolic acidosis can lead to acidemia, which is defined as arterial blood pH that is lower than 7.35. Acidemia and acidosis are not mutually exclusive – pH and hydrogen ion concentrations also depend on the coexistence of other acid-base disorders; therefore, pH levels in people with metabolic acidosis can range from low to high.
Acute metabolic acidosis, lasting from minutes to several days, often occurs during serious illnesses or hospitalizations, and is generally caused when the body produces an excess amount of organic acids (ketoacids in ketoacidosis, or lactic acid in lactic acidosis). A state of chronic metabolic acidosis, lasting several weeks to years, can be the result of impaired kidney function (chronic kidney disease) and/or bicarbonate wasting. The adverse effects of acute versus chronic metabolic acidosis also differ, with acute metabolic acidosis impacting the cardiovascular system in hospital settings, and chronic metabolic acidosis affecting muscles, bones, kidney and cardiovascular health.
Symptoms are not specific, and diagnosis can be difficult unless patients present with clear indications for blood gas sampling. Symptoms may include palpitations, headache, altered mental status such as severe anxiety due to hypoxia, decreased visual acuity, nausea, vomiting, abdominal pain, altered appetite and weight gain, muscle weakness, bone pain, and joint pain. People with acute metabolic acidosis may exhibit deep, rapid breathing called Kussmaul respirations which is classically associated with diabetic ketoacidosis. Rapid deep breaths increase the amount of carbon dioxide exhaled, thus lowering the serum carbon dioxide levels, resulting in some degree of compensation. Overcompensation via respiratory alkalosis to form an alkalemia does not occur.[citation needed]
Extreme acidemia can also lead to neurological and cardiac complications:[citation needed]
Physical examination can occasionally reveal signs of the disease, but is often otherwise normal. Cranial nerve abnormalities are reported in ethylene glycol poisoning, and retinal edema can be a sign of methanol intoxication.[citation needed]
Chronic metabolic acidosis has non-specific clinical symptoms but can be readily diagnosed by testing serum bicarbonate levels in patients with chronic kidney disease (CKD) as part of a comprehensive metabolic panel. Patients with CKD Stages G3–G5 should be routinely screened for metabolic acidosis.
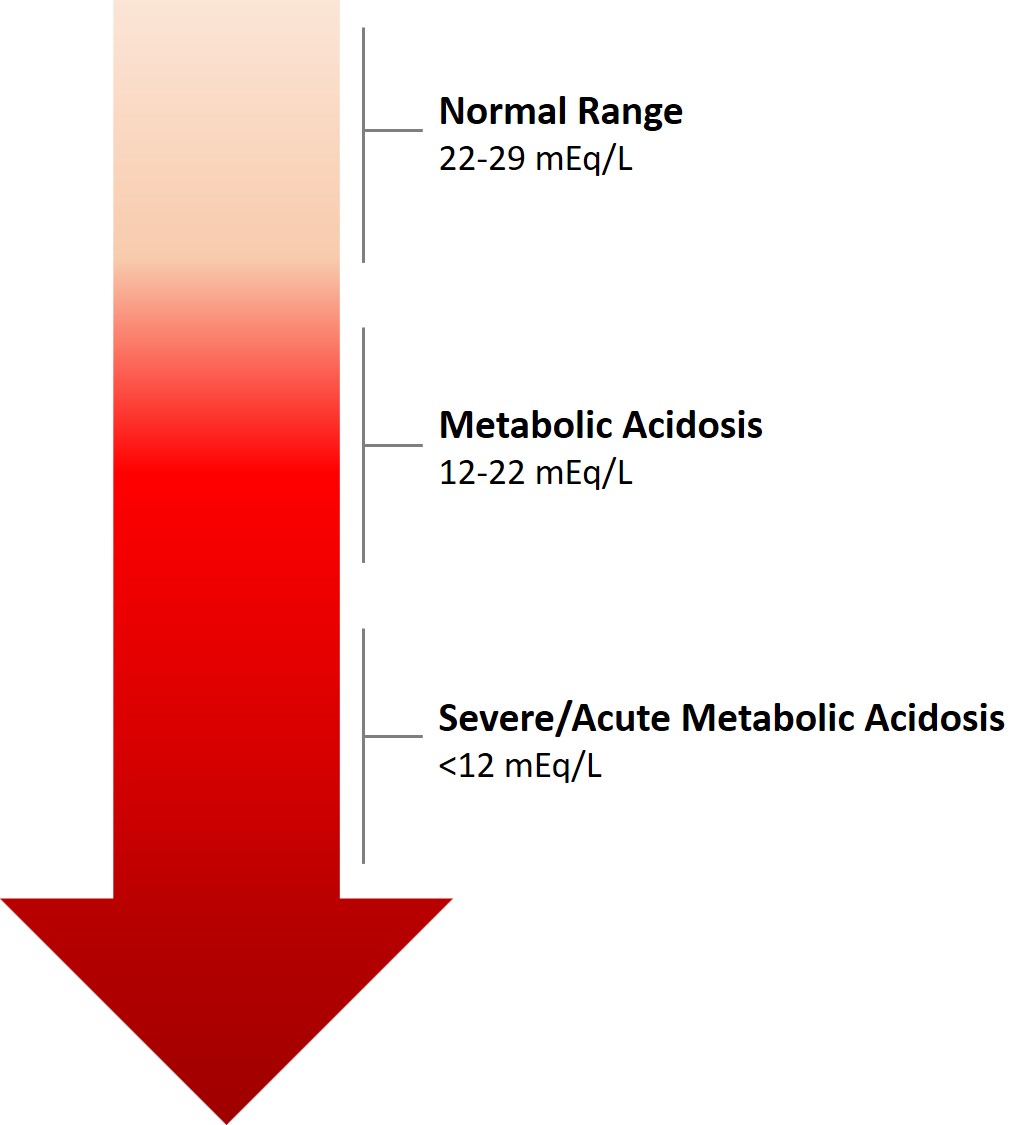
Metabolic acidosis results in a reduced serum pH that is due to metabolic and not respiratory dysfunction. Typically the serum bicarbonate concentration will be <22 mEq/L, below the normal range of 22 to 29 mEq/L, the standard base will be more negative than -2 (base deficit) and the pCO2 will be reduced as a result of hyperventilation in an attempt to restore the pH closer to normal. Occasionally in a mixed acid-base disorder where metabolic acidosis is not the primary disorder present, the pH may be normal or high. In the absence of chronic respiratory alkalosis, metabolic acidosis can be clinically diagnosed by analysis of the calculated serum bicarbonate level.[citation needed]
Generally, metabolic acidosis occurs when the body produces too much acid (e.g., lactic acidosis, see below section), there is a loss of bicarbonate from the blood, or when the kidneys are not removing enough acid from the body.[citation needed]
Hub AI
Metabolic acidosis AI simulator
(@Metabolic acidosis_simulator)
Metabolic acidosis
Metabolic acidosis is a serious electrolyte disorder characterized by an imbalance in the body's acid-base balance. Metabolic acidosis has three main root causes: increased acid production, loss of bicarbonate, and a reduced ability of the kidneys to excrete excess acids. Metabolic acidosis can lead to acidemia, which is defined as arterial blood pH that is lower than 7.35. Acidemia and acidosis are not mutually exclusive – pH and hydrogen ion concentrations also depend on the coexistence of other acid-base disorders; therefore, pH levels in people with metabolic acidosis can range from low to high.
Acute metabolic acidosis, lasting from minutes to several days, often occurs during serious illnesses or hospitalizations, and is generally caused when the body produces an excess amount of organic acids (ketoacids in ketoacidosis, or lactic acid in lactic acidosis). A state of chronic metabolic acidosis, lasting several weeks to years, can be the result of impaired kidney function (chronic kidney disease) and/or bicarbonate wasting. The adverse effects of acute versus chronic metabolic acidosis also differ, with acute metabolic acidosis impacting the cardiovascular system in hospital settings, and chronic metabolic acidosis affecting muscles, bones, kidney and cardiovascular health.
Symptoms are not specific, and diagnosis can be difficult unless patients present with clear indications for blood gas sampling. Symptoms may include palpitations, headache, altered mental status such as severe anxiety due to hypoxia, decreased visual acuity, nausea, vomiting, abdominal pain, altered appetite and weight gain, muscle weakness, bone pain, and joint pain. People with acute metabolic acidosis may exhibit deep, rapid breathing called Kussmaul respirations which is classically associated with diabetic ketoacidosis. Rapid deep breaths increase the amount of carbon dioxide exhaled, thus lowering the serum carbon dioxide levels, resulting in some degree of compensation. Overcompensation via respiratory alkalosis to form an alkalemia does not occur.[citation needed]
Extreme acidemia can also lead to neurological and cardiac complications:[citation needed]
Physical examination can occasionally reveal signs of the disease, but is often otherwise normal. Cranial nerve abnormalities are reported in ethylene glycol poisoning, and retinal edema can be a sign of methanol intoxication.[citation needed]
Chronic metabolic acidosis has non-specific clinical symptoms but can be readily diagnosed by testing serum bicarbonate levels in patients with chronic kidney disease (CKD) as part of a comprehensive metabolic panel. Patients with CKD Stages G3–G5 should be routinely screened for metabolic acidosis.
Metabolic acidosis results in a reduced serum pH that is due to metabolic and not respiratory dysfunction. Typically the serum bicarbonate concentration will be <22 mEq/L, below the normal range of 22 to 29 mEq/L, the standard base will be more negative than -2 (base deficit) and the pCO2 will be reduced as a result of hyperventilation in an attempt to restore the pH closer to normal. Occasionally in a mixed acid-base disorder where metabolic acidosis is not the primary disorder present, the pH may be normal or high. In the absence of chronic respiratory alkalosis, metabolic acidosis can be clinically diagnosed by analysis of the calculated serum bicarbonate level.[citation needed]
Generally, metabolic acidosis occurs when the body produces too much acid (e.g., lactic acidosis, see below section), there is a loss of bicarbonate from the blood, or when the kidneys are not removing enough acid from the body.[citation needed]
Recent media