
Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Medial epicondyle of the humerus
View on Wikipedia| Medial epicondyle of the humerus | |
|---|---|
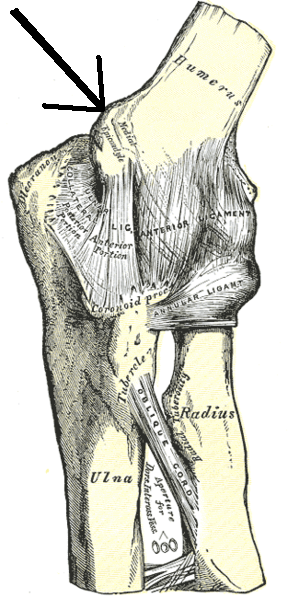
 Left elbow-joint, showing anterior and ulnar collateral ligaments. (Medial epicondyle labeled at center top.) | |
 Plan of ossification of the humerus. (Medial epicondyle labeled at lower left.) | |
| Details | |
| Identifiers | |
| Latin | epicondylus medialis humeri |
| TA98 | A02.4.04.027 |
| TA2 | 1207 |
| FMA | 23441 |
| Anatomical terms of bone | |
The medial epicondyle of the humerus is an epicondyle of the humerus bone of the upper arm in humans. It is larger and more prominent than the lateral epicondyle and is directed slightly more posteriorly in the anatomical position. In birds, where the arm is somewhat rotated compared to other tetrapods, it is called the ventral epicondyle of the humerus. In comparative anatomy, the more neutral term entepicondyle is used.
The medial epicondyle gives attachment to the ulnar collateral ligament of elbow joint, to the pronator teres, and to a common tendon of origin (the common flexor tendon) of some of the flexor muscles of the forearm: the flexor carpi radialis, the flexor carpi ulnaris, the flexor digitorum superficialis, and the palmaris longus. The medial epicondyle is located on the distal end of the humerus. Additionally, the medial epicondyle is inferior to the medial supracondylar ridge. It is also proximal to the olecranon fossa.
The medial epicondyle protects the ulnar nerve, which runs in a groove on the back of this epicondyle. The ulnar nerve is vulnerable because it passes close to the surface along the back of the bone. Striking the medial epicondyle causes a tingling sensation in the ulnar nerve. This response is known as striking the "funny bone".[1] The name funny bone could be from a play on the words humorous and humerus, the bone on which the medial epicondyle is located,[2] although according to the Oxford English Dictionary, it may refer to "the peculiar sensation experienced when it is struck".[3] Medial epicondyle fracture of the humerus are common when falling onto an outstretched hand.
Fractures
[edit]Medial epicondyle fractures are common elbow injuries in children. There is considerable controversy about their treatment, with uncertainty about whether surgery to restore the natural position of the bone is better than healing in a cast.
Additional images
[edit]-
 Right medial epicondyle colored in red.
Right medial epicondyle colored in red. -
 Left humerus. Anterior view.
Left humerus. Anterior view. -
 Front of the left forearm. Superficial muscles.
Front of the left forearm. Superficial muscles. -
 Posterior surface of the forearm. Deep muscles.
Posterior surface of the forearm. Deep muscles. -
 Elbow joint. Deep dissection. Posterior view.
Elbow joint. Deep dissection. Posterior view. -
 Elbow joint. Deep dissection. Posterior view.
Elbow joint. Deep dissection. Posterior view. -
 Elbow joint. Deep dissection. Posterior view.
Elbow joint. Deep dissection. Posterior view.





References
[edit]![]() This article incorporates text in the public domain from page 212 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 212 of the 20th edition of Gray's Anatomy (1918)
- ^ Saladin, Kenneth S. (2012). Anatomy & Physiology: The Unity of Form and Function. McGraw-Hill Publishing Co. ISBN 978-0071316385.
- ^ Hendrickson, Robert A. (2004). The Facts on File Encyclopedia of Word and Phrase Origins (Facts on File Writer's Library). New York: Checkmark Books. p. 281. ISBN 0-8160-5992-6.
- ^ "Welcome to the new OED Online : Oxford English Dictionary". Dictionary.oed.com. Retrieved 2012-03-20.
External links
[edit]- Anatomy figure: 07:02-02 at Human Anatomy Online, SUNY Downstate Medical Center
- Slim Golf Blog - Treating & Preventing Golfer's Elbow
- radiographsul at The Anatomy Lesson by Wesley Norman (Georgetown University) (xrayelbow)
{kind=link}