
Community hub
Gleason grading system
View on Wikipedia| Gleason grading system | |
|---|---|
 Gleason grade — Lower grades are associated with small, closely packed glands. Cells spread out and lose glandular architecture as grade increases. Gleason score is calculated from grade as described in the text. |
The Gleason grading system is used to help evaluate the prognosis of patients with prostate cancer using samples from a prostate biopsy. Together with other parameters, it is incorporated into a strategy of prostate cancer staging which predicts prognosis and helps guide therapy. A Gleason score is given to prostate cancer based upon its microscopic appearance.[1]
Cancers with a higher Gleason score are more aggressive and have a worse prognosis. Pathological scores range from 2 to 10, with higher numbers indicating greater risks and higher mortality. The system is widely accepted and used for clinical decision making even as it is recognised that certain biomarkers, like ACP1 expression, might yield higher predictive value for future disease course.[2]
The histopathologic diagnosis of prostate cancer has implications for the possibility and methodology of Gleason scoring.[3] For example, it is not recommended in signet-ring adenocarcinoma or urothelial carcinoma of the prostate, and the scoring should discount the foamy cytoplasms seen in foamy gland carcinoma.[3]
A total score is calculated based on how cells look under a microscope, with the first half of the score based on the dominant, or most common cell morphology (scored 1 to 5), and the second half based on the non-dominant cell pattern with the highest grade (scored 1 to 5). These two numbers are then combined to produce a total score for the cancer.
Specimens and processing
[edit]Most often, a urologist or radiologist will remove a cylindrical sample (biopsy) of prostate tissue through the rectum (or, sometimes the perineum), using hollow needles, and biomedical scientists in a histology laboratory prepare microscope slides for H&E staining and immunohistochemistry for diagnosis by a pathologist. If the prostate is surgically removed, a pathologist will slice the prostate for a final examination.[citation needed]
Histologic patterns
[edit]


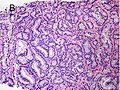
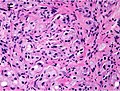
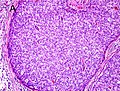
A pathologist microscopically examines the biopsy specimen for certain "Gleason" patterns. These Gleason patterns are associated with the following features:[citation needed]
- Pattern 1 – The cancerous prostate closely resembles normal prostate tissue. The glands are small, well-formed, and closely packed. This corresponds to a well differentiated carcinoma.
- Pattern 2 – The tissue still has well-formed glands, but they are larger and have more tissue between them, implying that the stroma has increased. This also corresponds to a moderately differentiated carcinoma.
- Pattern 3 – The tissue still has recognizable glands, but the cells are darker. At high magnification, some of these cells have left the glands and are beginning to invade the surrounding tissue or having an infiltrative pattern. This corresponds to a moderately differentiated carcinoma.
- Pattern 4 – The tissue has few recognizable glands. Many cells are invading the surrounding tissue in neoplastic clumps. This corresponds to a poorly differentiated carcinoma.
- Pattern 5 – The tissue does not have any or only a few recognizable glands. There are often just sheets of cells throughout the surrounding tissue. This corresponds to an anaplastic carcinoma.
In the present form of the Gleason system, prostate cancer of Gleason patterns 1 and 2 are rarely seen. Gleason pattern 3 is by far the most common.[citation needed]
Primary, secondary and tertiary grades
[edit]After analyzing the tissue samples, the pathologist then assigns a grade to the observed patterns of the tumor specimen.[citation needed]
- Primary grade – assigned to the dominant pattern of the tumor (has to be greater than 50% of the total pattern seen).
- Secondary grade – assigned to the next-most frequent pattern (has to be less than 50%, but at least 5%, of the pattern of the total cancer observed).
- Tertiary grade – increasingly, pathologists provide details of the "tertiary" component. This is where there is a small component of a third (generally more aggressive) pattern.
Scores and prognoses
[edit]The pathologist then sums the pattern-number of the primary and secondary grades to obtain the final Gleason score. If only two patterns are seen, the first number of the score is that of the tumor's primary grade while the second number is that of the secondary grade, as described in the previous section. If three patterns are seen, the first number of the score would be the primary grade and the second number the pattern with the highest grade.
For example, if the primary tumor grade was 2 and the secondary tumor grade was 3 but some cells were found to be grade 4, the Gleason score would be 2+4=6. This is a slight change from the pre-2005 Gleason system where the second number was the secondary grade (i.e., the grade of the second-most common cell line pattern).[4]
-
 Pattern 6 (3+3)
Pattern 6 (3+3) -
 Pattern 7 (3+4)
Pattern 7 (3+4) -
 Pattern 8 (4+4)
Pattern 8 (4+4) -
 Pattern 9 (4+5)
Pattern 9 (4+5) -
 Pattern 10 (5+5)
Pattern 10 (5+5)
.jpg)
.jpg)
.jpg)
.jpg)
.jpg)
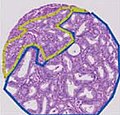
Key- blue: Gleason pattern 3 region, yellow: Gleason pattern 4 region, red: Gleason pattern 5 region
Gleason scores range from 2 to 10, with 2 representing the most well-differentiated tumors and 10 the least-differentiated tumors. Gleason scores have often been categorized into groups that show similar biologic behavior: low-grade (well-differentiated), intermediate-grade, moderate to poorly differentiated or high-grade.[5]
More recently, an investigation of the Johns Hopkins Radical Prostatectomy Database (1982–2011) led to the proposed reporting of Gleason grades and prognostic grade groups as:
- Gleason score ≤ 6 (prognostic grade group I);
- Gleason score 3+4=7 (prognostic grade group II) indicating the majority is pattern 3;
- Gleason score 4+3=7 (prognostic grade group III) where pattern 4 is dominant;[6]
- Gleason score 4+4=8 (prognostic grade group IV);
- Gleason scores 9–10 (prognostic grade group V).[7]
Prostate cancers with a Gleason score ≤ 6 usually have rather good prognoses.
Grading mechanism
[edit]The Gleason grade of architectural pattern is sometimes referred to as the Gleason architectural pattern.[citation needed]
The Gleason grade is based on tissue architectural patterns rather than purely cytological changes. These tissue patterns are classified into 5 grades, numbered 1 though 5. Lower numbers indicate more differentiation, with pattern 5 being the least differentiated.[4][7] Differentiation is the degree to which the tissue, in this case the tumor, resembles native tissue. Greater resemblance (lower grade) is typically associated with a better prognosis.[citation needed]
However, the Gleason score is not simply the highest grade (least differentiated) pattern within the tumor. Rather, it is a combination of the most two most frequent patterns seen. This recognizes that prostatic carcinomas have multiple patterns and that prognosis is more accurately determined by adding the scores of the two most prevalent patterns. Using this system, the grades of the most prevalent and second most prevalent patterns (if at least 5% of the total), are added together to yield the overall Gleason score.[4][7]
For example, if the most prevalent pattern/grade is 2, and the second most prevalent grade is 1, then the Gleason score is 2+1=3. If the neoplasm has only one pattern, the grade of that pattern is doubled to obtain the score. For example, if a tumor is entirely grade 1, the Gleason score would be 1+1=2. The most differentiated tumor would have the lowest score, Gleason 2 (1+1), while the most undifferentiated neoplasm (not resembling native prostate tissue) would have the highest score, Gleason 10 (5+5). Gleason scores range from 2 to 10; by definition there is no score of 0 or 1.[4][7]
Cytological differences between normal prostate and neoplastic glands are evident in changes to the typical two cell layers of the gland. In prostatic adenocarcinoma, the basal (bottom, usually cuboidal type) cell layer is lost, with only the top layer (usually columnar to pseudostratified) remaining.[citation needed]
-
 Gleason score 6 (3+3)
Gleason score 6 (3+3) -
 Cribriform pattern: Gleason grade 4
Cribriform pattern: Gleason grade 4 -
 Gleason score 7 (3+4) with minor component of cribriform glands
Gleason score 7 (3+4) with minor component of cribriform glands -
 Gleason score 8 (4+4) with glomeruloid glands
Gleason score 8 (4+4) with glomeruloid glands -
 Gleason score 8 (4+4) with irregular cribriform glands
Gleason score 8 (4+4) with irregular cribriform glands -
 Gleason score 8 (4+4) with fused glands with cytoplasmic vacuoles
Gleason score 8 (4+4) with fused glands with cytoplasmic vacuoles -
 Gleason score 8 (4+4) with poorly-formed glands
Gleason score 8 (4+4) with poorly-formed glands -
 Gleason score 9 (4+5) with cribriform glands, some with necrosis
Gleason score 9 (4+5) with cribriform glands, some with necrosis -
 Gleason score 10 (5+5) with cords of cells
Gleason score 10 (5+5) with cords of cells -
 Gleason score 10 (5+5) with individual cells
Gleason score 10 (5+5) with individual cells -
 Gleason score 10 (5+5) with solid sheets of cells
Gleason score 10 (5+5) with solid sheets of cells
.jpg)

_with_minor_component_of_cribriform_glands.jpg)
_with_glomeruloid_glands.jpg)
_with_irregular_cribriform_glands.jpg)
_with_fused_glands_with_cytoplasmic_vacuoles.jpg)
_with_poorly-formed_glands.jpg)
_with_cribriform_glands,_some_with_necrosis.jpg)
_with_cords_of_cells.jpg)
_with_individual_cells.jpg)
_with_solid_sheets_of_cells.jpg)
Score descriptions
[edit]Using this system, the most well-differentiated tumors have a Gleason score/grade of 2, and the least-differentiated tumors a score of 10. Range by definition is from 2 to 10, with architectural type from 1–5, and always added together or doubled, as described above. Gleason scores are often grouped together, based on similar behaviour: Grade 2–4 as well-differentiated, Grade 5–6 as intermediately-differentiated, Grade 7 as moderately to poorly differentiated (either 3+4=7, where the majority is pattern 3, or 4+3=7 in which pattern 4 dominates and indicates less differentiation,[6] and Grade 8–10 as "high-grade."[4][7]
Gleason 1
[edit]Gleason pattern 1 is the most well-differentiated tumor pattern. It is a well-defined nodule of single/separate, closely/densely packed, back-to-back gland pattern that does not invade into adjacent healthy prostatic tissue. The glands are round to oval shaped and proportionally large, compared to Gleason pattern 3 tumors, and are approximately equal in size and shape to one another.[4][7]
Gleason 2
[edit]Gleason 2 is fairly well-circumscribed nodules of single, separate glands. However, the glands are looser in arrangement and not as uniform as in pattern 1. Minimal invasion by neoplastic glands into the surrounding healthy prostate tissue may be seen. Similar to Gleason 1, the glands are usually larger than those of Gleason 3 patterns, and are round to oval in shape. Thus the main difference between Gleason 1 and 2 is the density of packing of the glands seen; invasion is possible in Gleason 2, but by definition not in Gleason 1.[4][7]
Gleason 3
[edit]Gleason 3 is a clearly infiltrative neoplasm, with extension into adjacent healthy prostate tissue. The glands alternate in size and shape, and are often long/angular. They are usually small/micro-glandular in comparison to Gleason 1 or 2 grades. However, some may be medium to large in size. The small glands of Gleason 3, in comparison to the small and poorly defined glands of pattern 4, are distinct glandular units. Mentally you could draw a circle around each of the glandular units in Gleason 3.[4][7]
Gleason 4
[edit]Gleason pattern 4 glands are no longer single/separated glands like those seen in patterns 1–3. They look fused together, difficult to distinguish, with rare lumen formation vs Gleason 1–3 which usually all have open lumens (spaces) within the glands, or can be cribriform-(resembling the cribriform plate/similar to a sieve: an item with many perforations). Fused glands are chains, nests, or groups of glands that are no longer entirely separated by stroma-(connective tissue that normally separates individual glands in this case). Fused glands contain occasional stroma giving the appearance of "partial" separation of the glands. Due to this partial separation, fused glands sometimes have a scalloped (think looking at a slice of bread with bite taken out of it) appearance at their edges.[4][7]
Gleason 5
[edit]Neoplasms have no glandular differentiation (thus not resembling normal prostate tissue at all). It is composed of sheets (groups of cells almost planar in appearance (like the top of a box), solid cords (group of cells in a rope like fashion running through other tissue/cell patterns seen), or individual cells. You should not see round glands with lumenal spaces that can be seen in the other types that resemble more the normal prostate gland appearance.[4][7]
Prognosis
[edit]Gleason scores 2–4 are typically found in smaller tumors located in the transitional zone (around the urethra). These are typically found incidentally on surgery for benign prostatic hyperplasia, which is not itself a precursor lesion for prostatic carcinoma.[4]
The majority of treatable/treated cancers are of Gleason scores 5–7 and are detected due to biopsy after abnormal digital rectal examination or prostate-specific antigen evaluation. The cancer is typically located in the peripheral zone usually the posterior portion, explaining the rationale of performing the digital rectal exam.[citation needed]
Tumors with Gleason scores 8–10 tend to be advanced neoplasms that are unlikely to be cured. Although some evidence suggests that prostate cancers will become more aggressive over time, Gleason scores typically remain stable for several years.[4]
The Gleason scores then become part of the TNM or Whitmore-Jewett prostate cancer staging system to provide prognosis.
History
[edit]The Gleason scoring system takes its name from Donald Gleason (1920–2008), a pathologist at the Minneapolis Veterans Affairs Hospital, who developed it with colleagues at that facility in the 1960s.[8][9] In 2005 the International Society of Urological Pathology altered the Gleason system, refining the criteria and changing the attribution of certain patterns.[4] It has been shown that this "modified Gleason score" has higher performance than the original one, and it is currently assumed standard in urological pathology. In this form, it remains an important tool.[10]
However, problematic aspects of the original Gleason grading system still characterize the 2005 revision. The predominant lowest score assigned is Gleason 3+3 = 6. Patients who are told their Gleason score is 6 out of 10 may interpret that they have a more aggressive intermediate cancer and experience greater anxiety.[11] More importantly, some classification systems fail to clearly distinguish between Gleason 3+4 = 7 and Gleason 4+3 = 7, with the latter having a worse prognosis.
Therefore, in 2014 an international multidisciplinary conference was convened to revise the 2005 system. A 5-point Gleason Grade grouping similar to those such as PI-RADS used with prostate MRI evaluations was proposed to denote prognostically distinct stratification. Grade 1 would indicate the lowest-risk cancer while Grade 5 would indicate the most aggressive disease. The system was tested and validated against 20,000 prostatectomy specimens and at least 16,000 biopsy samples.
The majority of conference participants concurred on the superiority of the scale over the 2005 Gleason grading system, pointing to the likelihood that overtreatment could be avoided for those patients whose cancer was assigned Grade 1. The World Health Organization's 2016 edition of Pathology and Genetics: Tumours of the Urinary System and Male Genital Organs has accepted the 2014 system, which can be used in conjunction with the 2005 Gleason system.[12]
See also
[edit]References
[edit]- ^ "Male Genital Pathology". The Internet Pathology Laboratory for Medical Education. The University of Utah, Eccles Health Sciences Library. Retrieved 2009-05-13.
- ^ Ruela-de-Sousa RR, Hoekstra E, Hoogland AM, Souza Queiroz KC, Peppelenbosch MP, Stubbs AP, et al. (April 2016). "Low-Molecular-Weight Protein Tyrosine Phosphatase Predicts Prostate Cancer Outcome by Increasing the Metastatic Potential". European Urology. 69 (4): 710–719. doi:10.1016/j.eururo.2015.06.040. hdl:1765/79946. PMID 26159288.
- ^ a b Li J, Wang Z (February 2016). "The pathology of unusual subtypes of prostate cancer". Chinese Journal of Cancer Research = Chung-Kuo Yen Cheng Yen Chiu. 28 (1): 130–143. doi:10.3978/j.issn.1000-9604.2016.01.06. PMC 4779761. PMID 27041935.
- ^ a b c d e f g h i j k l m Epstein JI, Allsbrook WC, Amin MB, Egevad LL (September 2005). "The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma". The American Journal of Surgical Pathology. 29 (9): 1228–1242. doi:10.1097/01.pas.0000173646.99337.b1. PMID 16096414. S2CID 7428768.
- ^ Kumar V, Abbas AK, Fausto N. Robbins and Cotran Pathologic Basis of Disease. Seventh ed: Elsevier Saunders; 2005.
- ^ a b Humphrey PA (March 2004). "Gleason grading and prognostic factors in carcinoma of the prostate". Modern Pathology. 17 (3): 292–306. doi:10.1038/modpathol.3800054. PMID 14976540.
- ^ a b c d e f g h i j Pierorazio PM, Walsh PC, Partin AW, Epstein JI. Prognostic Gleason grade grouping: data based on the modified Gleason scoring system. BJU International. 2013;111(5):753–760.
- ^ Albertsen, Peter C. (1 May 2006). "How to interpret Gleason score in contemporary biopsy". Urology Times. Archived from the original on 2006-11-23. (URL is live, but appear corrupted compared to archived version.)
- ^ Gleason DF (1977). "The Veteran's Administration Cooperative Urologic Research Group: histologic grading and clinical staging of prostatic carcinoma". In Tannenbaum M (ed.). Urologic Pathology: The Prostate. Philadelphia: Lea and Febiger. pp. 171–198. ISBN 0-8121-0546-X.
- ^ Brimo F, Montironi R, Egevad L, Erbersdobler A, Lin DW, Nelson JB, et al. (May 2013). "Contemporary grading for prostate cancer: implications for patient care". European Urology. 63 (5): 892–901. doi:10.1016/j.eururo.2012.10.015. PMID 23092544.
- ^ McCullough M (December 13, 2015). "More with early-stage prostate cancers choosing to wait and see before surgery". The Philadelphia Inquirer. (related, from philly.com: 8 tell how they handle testing, anxiety of prostate cancer waiting)
- ^ Sperling D. "Revisions of the Gleason grading system make it more accurate". Sperling Prostate Center. Retrieved 31 March 2016.
External links
[edit]- Thorson P, Humphrey PA (December 2000). "Minimal adenocarcinoma in prostate needle biopsy tissue". American Journal of Clinical Pathology. 114 (6): 896–909. doi:10.1309/KVPX-C1EM-142L-1M6W. PMID 11338479. Pathology slides and explanation. [Free]
- WHO, Geneva Foundation for Medical Education and Research, Prostate cancer, Gleason score. 51 images.
Gleason grading system
View on GrokipediaOverview
Definition and Purpose
The Gleason grading system is a histological classification method for assessing the aggressiveness of prostate adenocarcinoma through microscopic evaluation of glandular architectural patterns in tissue specimens. It utilizes a five-tier scale, designated as Grades 1 through 5, which quantifies the degree to which malignant glands deviate from the normal, well-formed structure of benign prostate tissue; Grade 1 represents nearly normal architecture, while Grade 5 indicates complete loss of glandular differentiation and highly disorganized growth.[1][6] This purely morphological approach focuses on the spatial arrangement and architectural features of tumor cells, enabling pathologists to categorize the tumor's potential for progression based on observable deviations in biopsy or surgical samples.[2] Developed by pathologist Donald F. Gleason in 1966 specifically for prostatic carcinoma, the system provides a standardized framework for grading that correlates directly with tumor behavior.[1][7] The primary purpose of the Gleason grading system is to predict prostate cancer's clinical behavior and prognosis by informing the interpretation of biopsy results, thereby guiding treatment decisions such as active surveillance, surgery, or radiation therapy.[2][7] Unlike molecular or genetic assays, it relies solely on routine histopathological examination, making it accessible and integral to risk stratification in clinical practice without additional specialized testing.[2]Clinical Significance
The Gleason grading system plays a pivotal role in stratifying prostate cancer into low-, intermediate-, and high-risk categories, primarily based on the histologic grade derived from biopsy or prostatectomy specimens. Low-risk disease, typically corresponding to Gleason scores of 6 or less (Grade Group 1), is characterized by indolent behavior and often managed with active surveillance to avoid overtreatment. Intermediate-risk cases (Gleason score 7, Grade Groups 2-3) may involve a mix of favorable and unfavorable features, guiding decisions toward radical prostatectomy, external beam radiation therapy, or brachytherapy, sometimes combined with short-term androgen deprivation therapy. High-risk prostate cancer (Gleason scores 8-10, Grade Groups 4-5) indicates aggressive disease requiring multimodal approaches, such as surgery followed by adjuvant radiation or long-term hormone therapy, to optimize local control and reduce recurrence risk.[2][8] Higher Gleason grades are strongly correlated with increased risk of metastasis and poorer clinical outcomes, as they reflect more poorly differentiated tumor architecture prone to invasion and spread. For instance, patients with low-grade tumors (Gleason ≤6) exhibit a 5-year relative survival rate exceeding 99% when localized, underscoring the favorable prognosis. In contrast, high-grade tumors (Gleason 8-10) are associated with a substantially elevated metastasis risk, contributing to 5-year survival rates dropping to approximately 30-37% in cases with distant spread, which is more common in advanced high-grade disease.[9][2] The Gleason score is integrated with prostate-specific antigen (PSA) levels and tumor volume metrics in validated risk assessment models to refine prognosis and personalize management. The Cancer of the Prostate Risk Assessment (CAPRA) score incorporates Gleason grade, PSA, clinical stage, percentage of positive biopsy cores, and age to predict biochemical recurrence and metastasis-free survival, with scores of 0-2 indicating low risk and 6-10 high risk. Similarly, Memorial Sloan Kettering Cancer Center (MSKCC) nomograms combine Gleason score, PSA, and clinical stage to estimate pathologic outcomes post-prostatectomy and guide adjuvant therapy decisions, enhancing predictive accuracy over Gleason alone.[10]History
Original Development
The Gleason grading system was developed by pathologist Donald F. Gleason at the University of Minnesota during 1966–1967, drawing on his analysis of 270 radical prostatectomy specimens collected as part of the Veterans Administration Cooperative Urological Research Group (VACURG) studies.[1][11] These specimens provided a comprehensive dataset of prostate cancer cases treated at Veterans Administration hospitals, enabling Gleason to identify consistent histological patterns associated with disease progression and survival.[1][11] Gleason's initial publication in 1966 introduced the system in Cancer Chemotherapy Reports, where he outlined five grades (1 through 5) based solely on the architectural organization of tumor glands observed under low-power microscopy (4× to 10× magnification).[1] This approach emphasized the degree of glandular differentiation and structural disruption, correlating these patterns directly with clinical outcomes from the VACURG cohort, such as survival rates and metastasis risk.[1] A companion paper in the same issue detailed survival data, demonstrating the prognostic utility of the grades. The core intent of the system was to establish a highly reproducible method for grading prostate adenocarcinoma that relied exclusively on architectural features, excluding subjective cytological details like nuclear atypia or cell size to minimize interobserver variability.[1] By focusing on glandular formation—from well-formed, closely packed glands in grade 1 to complete loss of architecture in grade 5—Gleason aimed to provide pathologists with objective criteria that could predict tumor behavior more reliably than prior systems.[1] This architecture-centric design proved foundational, as validated in a 1967 follow-up study in The Journal of Urology that further linked grades to long-term prognosis in the VACURG patients.[12]Major Updates and Revisions
In 1974, Gleason and Mellinger expanded the original study to 1,032 patients from the VACURG series, confirming the strong prognostic correlations between combined histological grading and clinical staging with outcomes such as survival.[13] In 1977, Donald Gleason further refined the system by emphasizing low-power magnification for pattern assessment and clarifying that tertiary (third) patterns, when comprising less than 5% of the tumor, should generally not alter the primary and secondary grade assignment, thereby eliminating their routine use in most cases to enhance reproducibility.[14] The 2005 International Society of Urological Pathology (ISUP) consensus conference introduced significant modifications, reclassifying most cribriform and mucinous patterns as Gleason grade 4 due to their association with adverse outcomes, while restricting grade 2 to rare, well-circumscribed small nodules and discontinuing grades 2 and 3 as primary patterns in needle biopsies to reduce undergrading.[15] Building on prior updates, the 2014 ISUP consensus conference, with further refinements in 2016, proposed a simplified 5-tier Grade Group system—mapping Gleason scores 6 (3+3), 7 (3+4), 7 (4+3), 8 (4+4), and 9-10 to Grade Groups 1 through 5, respectively—to better correlate with prostate cancer prognosis and facilitate clinical decision-making.[4] This framework was endorsed by the World Health Organization in its 2016 classification of genitourinary tumors.[16] By 2025, reaffirmations of the Grade Group system emerged through AI-assisted validation studies in digital pathology, confirming the system's robustness in contemporary workflows.[17] Recent developments in 2025 have further integrated digital pathology platforms with artificial intelligence for automated Gleason grading, enabling real-time analysis of whole-slide images to minimize subjectivity and interobserver variability in pattern recognition.[18] These AI models, trained on large datasets of annotated prostate biopsies, achieve diagnostic accuracies comparable to expert pathologists while providing explainable outputs aligned with ISUP criteria, supporting their adoption in clinical practice for improved efficiency and equity in grading.[19]Specimen Acquisition and Processing
Types of Specimens
The Gleason grading system is applied to various types of prostate tissue specimens obtained through different clinical procedures, each with distinct acquisition methods that influence the accuracy and representativeness of the grading assessment.[20] Needle biopsies represent the most common specimen type for initial prostate cancer diagnosis and Gleason grading, typically obtained via transrectal ultrasound-guided (TRUS) or transperineal approaches under local anesthesia. Contemporary protocols often incorporate MRI-targeted sampling, such as MRI-ultrasound fusion or cognitive guidance, to focus on suspicious lesions identified on pre-biopsy multiparametric MRI, alongside systematic cores.[21][22] These procedures yield multiple small cylindrical cores of tissue, usually 10 to 12 in standard extended sampling or up to 18 in saturation biopsies, targeting the peripheral zone where most cancers arise.[23] However, due to the limited volume of each core (typically 10-20 mm in length) and the multifocal, heterogeneous nature of prostate cancer, needle biopsies are prone to sampling error, potentially missing higher-grade areas.[24] Transurethral resection of the prostate (TURP) specimens are obtained during surgical treatment for symptomatic benign prostatic obstruction, such as lower urinary tract symptoms from hyperplasia, and incidentally reveal cancer in about 5-10% of cases.[25] Unlike needle cores, TURP provides larger volumes of tissue through electrosurgical resection via the urethra, resulting in multiple fragmented chips from the transitional zone, which may include a different distribution of cancer patterns compared to peripheral zone biopsies.[26] These fragments allow for broader sampling but can complicate architectural assessment due to their irregular, non-contiguous nature.[27] Radical prostatectomy specimens offer the most comprehensive tissue for Gleason grading, involving the entire resected prostate gland following surgical removal for clinically localized cancer.[28] This whole-gland analysis enables detailed sectioning and evaluation of all tumor foci, providing a definitive grade but only retrospectively after definitive treatment.[29] In comparisons of sampling adequacy, needle biopsies underestimate the final Gleason score in approximately 20-40% of cases relative to radical prostatectomy findings, primarily due to intratumoral heterogeneity where higher-grade components may be undersampled.[30] TURP specimens, while less affected by peripheral zone undersampling, can still miss occult disease in unsampled regions.[31]Laboratory Preparation Techniques
The laboratory preparation of prostate tissue specimens for Gleason grading begins with fixation to preserve the architectural features essential for evaluating glandular patterns. Prostate needle biopsies are typically fixed in 10% neutral buffered formalin (NBF) immediately after collection to prevent autolysis and maintain tissue morphology.[32] The recommended fixation duration is 24-48 hours, allowing adequate penetration for thin biopsy cores (approximately 1 mm in diameter) while minimizing degradation; shorter times (8-24 hours) may suffice for optimal immunohistochemical performance, but extended immersion up to 72 hours ensures stability for fluorescence in situ hybridization if needed.[33] Overfixation beyond 72 hours should be avoided, as it can lead to tissue hardening, shrinkage, and artifactual distortion of glandular structures, potentially complicating pattern recognition.[34] Following fixation, the tissue undergoes dehydration in graded alcohols, clearing with xylene, and embedding in paraffin wax to create durable blocks for long-term storage and sectioning. Sections are cut at 4-5 microns thickness using a microtome, a standard depth that balances resolution of cellular details with prevention of tearing in fibrous prostate stroma.[35] These sections are then mounted on glass slides and stained with hematoxylin and eosin (H&E), where hematoxylin highlights nuclei and eosin stains cytoplasm and extracellular matrix, enabling visualization of the cribriform, fused, or individual glandular architectures critical to Gleason assessment.[32] In cases where H&E staining yields ambiguous findings, such as small foci of atypical glands or distinction between benign prostatic hyperplasia and low-grade carcinoma, adjunct immunohistochemistry is employed. A cocktail of p63 (a basal cell marker) and AMACR (alpha-methylacyl-CoA racemase, a positive marker for prostatic adenocarcinoma) is particularly useful, with p63 highlighting intact basal layers in benign tissue and AMACR showing overexpression in malignant cells, improving diagnostic accuracy in up to 95% of challenging biopsies.[36] This approach is recommended by consensus guidelines for resolving equivocal patterns without altering the primary H&E-based Gleason evaluation.[34] Quality control measures are integral to address prostate cancer's intratumoral heterogeneity, ensuring representative sampling across multiple cores (typically 12-14 per procedure). Biopsies should be processed site-specifically, with no more than two cores per cassette to minimize fragmentation and preserve core integrity for accurate quantitation of tumor involvement; this facilitates even examination of all regions, reducing undersampling risks that could underestimate aggressive patterns.[37] Adherence to these protocols, as outlined in standardized reporting guidelines, enhances reproducibility and reliability in Gleason grading.[38]Histological Patterns
Architectural Features by Grade
The Gleason grading system classifies prostate adenocarcinoma based on the architectural patterns of glandular structures observed under low-power microscopy, with grades ranging from 1 to 5 reflecting increasing deviation from normal prostate histology.[2] Grade 1 tumors are exceedingly rare and characterized by well-circumscribed nodules composed of uniform, closely packed glands that closely resemble normal prostate tissue, featuring discrete, well-differentiated glands of moderate size with minimal stromal separation.[39] These patterns are often indistinguishable from benign conditions like adenosis and are no longer routinely assigned in contemporary practice due to their near-normal appearance and lack of clinical significance.[2] Grade 2 Gleason pattern 2, characterized by moderately separated but organized glands, is rarely used in current practice following the 2005 and 2014 ISUP consensus updates, which discourage its assignment due to poor reproducibility and limited prognostic distinction from pattern 3. Consequently, historical or atypical reports using pattern 2 (e.g., 2+4 with tertiary 5) are interpreted in the context of modern grading, often aligning with Grade Group 2 equivalents when pattern 4 predominates secondary.[4][39] Grade 3, the most common pattern in low-grade prostate cancers, consists of infiltrative, smaller neoplastic glands that vary in size and shape, maintaining individual, discrete structures amidst benign stroma without extensive fusion.[2] These glands demonstrate moderate architectural distortion, with some irregularity but preservation of overall glandular lumina.[39] Grade 4 represents an intermediate- to high-risk pattern in prostate cancer, characterized by a heterogeneous group of histological subtypes including poorly formed glands, fused glands, cribriform glands, and glomeruloid structures, indicating a significant loss of individual glandular organization and associated with increased tumor aggressiveness and higher risk of metastasis, particularly the cribriform subtype which is linked to poorer clinical outcomes.[40][41] These features often manifest as poorly formed glands fused into irregular cribriform sheets, hypernephroid clusters, or ill-defined masses.[2] Post-2005 ISUP updates reclassified most cribriform patterns and glomeruloid structures as grade 4, emphasizing broad, irregular bridging and absence of well-defined lumina.[39] Grade 5 displays complete absence of glandular formation, manifesting as solid sheets, cords, or single infiltrating tumor cells, frequently accompanied by comedo-type necrosis within any residual cribriform or solid nests.[39] This highly disorganized architecture underscores the most aggressive behavior among graded patterns.[2]Pattern Recognition Criteria
Pattern recognition in the Gleason grading system involves evaluating the architectural arrangement of malignant glands under microscopy, focusing on their size, shape, spacing, and relationship to surrounding stroma and benign tissues to distinguish between grades. Higher-grade patterns are identified by their infiltrative growth, where tumor glands breach and disrupt the orderly arrangement of benign prostate acini or extend into adjacent structures such as fat, indicating loss of normal glandular circumscription.[28] For instance, Gleason pattern 4 is recognized by poorly formed or fused glands that infiltrate raggedly between residual benign glands, lacking the uniform nesting seen in lower grades.[42] In specimens with mixed patterns, accurate grading requires quantifying the relative proportions of each component to determine the dominant and secondary patterns. Consensus guidelines recommend that minor high-grade components constituting less than 5% of the tumor volume should not alter the primary score but may be noted separately; however, if a higher-grade pattern, such as grade 4 or 5, exceeds 5%, it typically upgrades the overall assessment to reflect the aggressive potential.[43] This threshold-based approach helps standardize reporting, particularly in needle biopsies where sampling may capture heterogeneous tumor areas. Common pitfalls in pattern recognition arise from benign mimics that simulate malignant architecture, leading to potential over- or under-grading. Conditions such as partial atrophy can present with shrunken, crowded glands resembling Gleason pattern 3 or 4, while seminal vesicle invasion may be confounded by the organ's pseudostratified epithelium mimicking high-grade carcinoma.[44] Additionally, interobserver variability remains a challenge, with studies reporting kappa values as low as 0.4-0.6 for grade assignments, though adoption of ISUP consensus guidelines has improved agreement by providing standardized criteria for ambiguous cases.[45] To aid recognition, pathologists employ low-power magnification (typically 4x to 10x) to evaluate overall glandular architecture and infiltration patterns, switching to higher power (20x to 40x) for confirming subtle features like gland fusion without relying on cytological atypia, as Gleason grading prioritizes morphology over nuclear details.[28] These practices minimize errors in distinguishing patterns, complementing the architectural definitions outlined in prior sections on grade features.Grading Procedure
Identifying Dominant Patterns
Pathologists begin the identification of dominant patterns in the Gleason grading system by systematically examining the entire histological slide of the prostate specimen, typically a biopsy core or radical prostatectomy section, under low magnification (4x to 10x objective) to map out tumor areas and assess overall architecture.[46] This initial low-power scan allows for the localization of malignant glandular structures amid benign prostate tissue, enabling a comprehensive overview of the tumor's spatial distribution and heterogeneity before higher magnification evaluation of specific patterns.[6] The primary pattern is selected as the architectural grade that occupies the most extensive area within the tumor.[2] This predominant pattern, which reflects the tumor's dominant growth behavior, is assigned a Gleason grade from 1 to 5 based on its glandular differentiation and architectural features, such as the size, shape, and arrangement of malignant glands.[2] If the tumor exhibits a single uniform pattern, that grade serves as both primary and secondary.[47] The secondary pattern is identified as the next most common architectural grade present in the tumor, even if it constitutes less than the primary, provided it is not overshadowed by a tertiary pattern of higher grade.[2] In cases where multiple patterns coexist, the secondary is the one with the second-largest proportional involvement, contributing to the overall representation of tumor diversity without exceeding the primary in extent.[6] Pathologists quantify these proportions visually during microscopic review, often estimating percentages to ensure accurate dominance assignment.[48] Tumor heterogeneity, common in prostate cancer, is addressed by prioritizing the worst (highest-grade) pattern observed, particularly if it appears focally within any biopsy core, as this may indicate aggressive subclones that influence the final grade despite limited representation.[38] In multi-core biopsies, each core is evaluated separately to detect such focal high-grade elements, with the highest-grade pattern across all cores potentially upgrading the overall assessment to reflect the most aggressive component.[20] This approach ensures that even minor but prognostically significant patterns are not overlooked, aligning with consensus guidelines from the International Society of Urological Pathology.[4]Assigning Primary and Secondary Grades
In the Gleason grading system, the primary grade is assigned to the architectural pattern that occupies the largest volume of the tumor.[28] The secondary grade is then assigned to the pattern with the second highest volume, which may be of a lower or higher grade than the primary, ensuring that the grading reflects the dominant histological features.[20] This assignment prioritizes volume-based prevalence in radical prostatectomy specimens, while needle biopsies emphasize the inclusion of the highest-grade pattern as secondary if it is not the most prevalent, to better capture tumor aggressiveness. When a tumor exhibits only a single dominant architectural pattern, the primary grade is doubled to form the secondary grade, resulting in a combined score such as 3+3=6 for a pure pattern 3 tumor.[28] This convention, established in the original system and reaffirmed in subsequent updates, avoids undergrading by treating the uniform pattern as both primary and secondary components. Tertiary patterns, representing a third distinct architectural component, are generally ignored in grade assignment unless they constitute a high-grade pattern (such as 4 or 5) and exceed 5% of the tumor volume in radical prostatectomy specimens, in which case they may upgrade the secondary grade.[28] In needle biopsies, however, any high-grade tertiary pattern is incorporated by assigning it as the secondary grade if it is the highest grade present, regardless of its minor volume, to ensure prognostic accuracy; patterns below 5% are otherwise noted separately without altering the core score. This approach stems from the 2005 International Society of Urological Pathology (ISUP) consensus, which aimed to standardize reporting while highlighting clinically significant minor high-grade elements.[20] Grading is conventionally reported in the format of primary grade plus secondary grade (e.g., 4+3), with the primary always listed first to denote the dominant pattern; separate scores are provided for distinct tumor nodules if multiple are present.[28] This notation facilitates clear communication in pathology reports and integration with clinical decision-making.Scoring Systems
Traditional Gleason Score Calculation
The traditional Gleason score is calculated by summing the primary grade, which represents the most prevalent architectural pattern in the tumor, and the secondary grade, which denotes the second most common pattern. In needle biopsies, even small amounts of a higher-grade pattern are graded as secondary to capture aggressive components; in surgical specimens, higher-grade patterns comprising less than 5% are typically reported as tertiary patterns without affecting the primary/secondary score. This summation yields a score ranging from 2 to 10, where the primary and secondary grades each range from 1 to 5 based on the degree of glandular differentiation and architectural disorganization observed histologically.[2][20] In contemporary practice, Gleason scores below 6 are no longer assigned, reflecting modifications from the 2005 International Society of Urological Pathology (ISUP) consensus conference, which discontinued the use of scores 2 through 5 on needle biopsies to improve prognostic accuracy and standardization. Originally described by Donald Gleason in the 1960s and 1970s, the system allowed for these lower scores, but the consensus emphasized that patterns corresponding to grades 1 and 2 are rarely identifiable in modern biopsies and do not represent clinically significant cancer when present. As a result, reported scores now typically range from 6 to 10, with the score expressed in the format "primary + secondary = total," such as 3+3=6 or 4+5=9.[49] This reporting convention provides nuanced assessment by preserving the individual grade components alongside the total score, allowing pathologists and clinicians to evaluate the relative contributions of each pattern—for instance, distinguishing a 3+4=7 (where grade 3 predominates) from a 4+3=7 (where grade 4 predominates). The primary and secondary grades are assigned after identifying the dominant histological patterns in the specimen, as detailed in the grading procedure.[2][20]ISUP Grade Groups
The International Society of Urological Pathology (ISUP) introduced a simplified 5-tier grading system in 2014 to address limitations in the traditional Gleason scoring, providing a more intuitive framework for communicating prostate cancer prognosis to clinicians and patients. This system, known as ISUP Grade Groups, stratifies tumors into prognostically distinct categories based on Gleason patterns, emphasizing clinical relevance over the original 2-10 scale. The grade groups were proposed by Epstein and validated across large multi-institutional cohorts, demonstrating superior predictive accuracy for outcomes compared to traditional scores. The ISUP Grade Groups correspond to specific Gleason score ranges as follows:| Grade Group | Gleason Score Equivalent | Risk Category |
|---|---|---|
| 1 | ≤6 | Low (indolent) |
| 2 | 3+4=7 | Favorable intermediate |
| 3 | 4+3=7 | Unfavorable intermediate |
| 4 | 8 | High |
| 5 | 9-10 | Very high |