Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
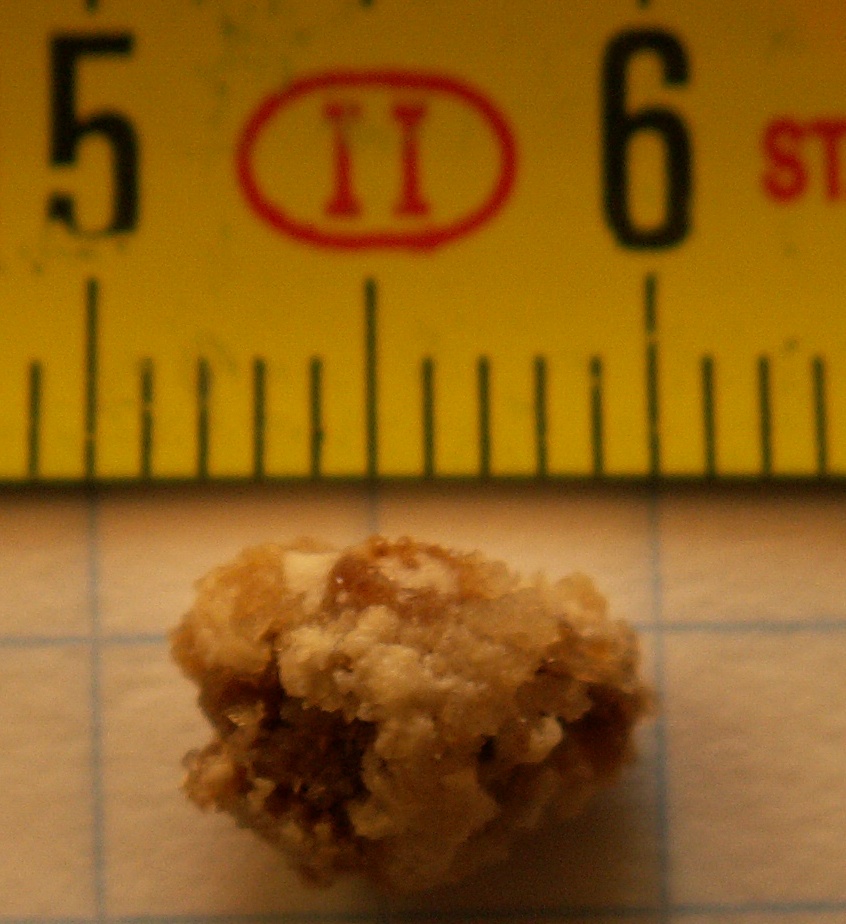
Kidney stone disease
Kidney stone disease or urinary stone disease is a crystallopathy that occurs when there are too many minerals in the urine and not enough liquid or hydration. This imbalance causes tiny pieces of crystal to aggregate and form hard masses, or calculi (stones) in the upper urinary tract. Because renal calculi typically form in the kidney, if small enough, they are able to leave the urinary tract via the urine stream. A small calculus may pass without causing symptoms. However, if a stone grows to more than 5 millimeters (0.2 inches), it can cause a blockage of the ureter, resulting in extremely sharp and severe pain (renal colic) in the lower back that often radiates downward to the groin. A calculus may also result in blood in the urine, vomiting (due to severe pain), swelling of the kidney, or painful urination. About half of all people who have had a kidney stone are likely to develop another within ten years.
Renal is Latin for "kidney", while nephro is the Greek equivalent. Lithiasis (Gr.) and calculus (Lat.- pl. calculi) both mean stone.
Most calculi form by a combination of genetics and environmental factors. Risk factors include high urine calcium levels, obesity, certain foods, some medications, calcium supplements, gout, hyperparathyroidism, and not drinking enough fluids. Calculi form in the kidney when minerals in urine are at high concentrations. The diagnosis is usually based on symptoms, urine testing, and medical imaging. Blood tests may also be useful. Calculi are typically classified by their location, being referred to medically as nephrolithiasis (in the kidney), ureterolithiasis (in the ureter), or cystolithiasis (in the bladder). Calculi are also classified by what they are made of, such as from calcium oxalate, uric acid, struvite, or cystine.
In those who have had renal calculi, drinking fluids, especially water, is a way to prevent them. Drinking fluids such that more than two liters of urine are produced per day is recommended. If fluid intake alone is not effective to prevent renal calculi, the medications thiazide diuretic, citrate, or allopurinol may be suggested. Soft drinks containing phosphoric acid (typically colas) should be avoided. When a calculus causes no symptoms, no treatment is needed. For those with symptoms, pain control is usually the first measure, using medications such as nonsteroidal anti-inflammatory drugs or opioids.[needs update] Larger calculi may be helped to pass with the medication tamsulosin, or may require procedures for removal such as extracorporeal shockwave therapy (ESWT), laser lithotripsy (LL), or a percutaneous nephrolithotomy (PCNL).
Renal calculi have affected humans throughout history with a description of surgery to remove them dating from as early as 600 BC in ancient India by Sushruta. Between 1% and 15% of people globally are affected by renal calculi at some point in their lives. In 2015, 22.1 million cases occurred, resulting in about 16,100 deaths. They have become more common in the Western world since the 1970s. Generally, more men are affected than women. The prevalence and incidence of the disease rises worldwide and continues to be challenging for patients, physicians, and healthcare systems alike. In this context, epidemiological studies are striving to elucidate the worldwide changes in the patterns and the burden of the disease and identify modifiable risk factors that contribute to the development of renal calculi.
The hallmark of a stone that obstructs the ureter or renal pelvis is excruciating, intermittent pain that radiates from the flank to the groin or to the inner thigh. This is due to the transfer of referred pain signals from the lower thoracic splanchnic nerves to the lumbar splanchnic nerves as the stone passes down from the kidney or proximal ureter to the distal ureter. This pain, known as renal colic, is often described as one of the strongest pain sensations known. Renal colic caused by kidney stones is commonly accompanied by urinary urgency, restlessness, frequent urination, blood in the urine, sweating, nausea, and vomiting. It typically comes in waves lasting 20 to 60 minutes caused by peristaltic contractions of the ureter as it attempts to expel the stone.
The embryological link between the urinary tract, the genital system, and the gastrointestinal tract is the basis of the radiation of pain to the gonads, as well as the nausea and vomiting that are also common in urolithiasis. Postrenal azotemia and hydronephrosis can be observed following the obstruction of urine flow through one or both ureters.
Pain in the lower-left quadrant can sometimes be confused with diverticulitis because the sigmoid colon overlaps the ureter, and the exact location of the pain may be difficult to isolate due to the proximity of these two structures.
Hub AI
Kidney stone disease AI simulator
(@Kidney stone disease_simulator)
Kidney stone disease
Kidney stone disease or urinary stone disease is a crystallopathy that occurs when there are too many minerals in the urine and not enough liquid or hydration. This imbalance causes tiny pieces of crystal to aggregate and form hard masses, or calculi (stones) in the upper urinary tract. Because renal calculi typically form in the kidney, if small enough, they are able to leave the urinary tract via the urine stream. A small calculus may pass without causing symptoms. However, if a stone grows to more than 5 millimeters (0.2 inches), it can cause a blockage of the ureter, resulting in extremely sharp and severe pain (renal colic) in the lower back that often radiates downward to the groin. A calculus may also result in blood in the urine, vomiting (due to severe pain), swelling of the kidney, or painful urination. About half of all people who have had a kidney stone are likely to develop another within ten years.
Renal is Latin for "kidney", while nephro is the Greek equivalent. Lithiasis (Gr.) and calculus (Lat.- pl. calculi) both mean stone.
Most calculi form by a combination of genetics and environmental factors. Risk factors include high urine calcium levels, obesity, certain foods, some medications, calcium supplements, gout, hyperparathyroidism, and not drinking enough fluids. Calculi form in the kidney when minerals in urine are at high concentrations. The diagnosis is usually based on symptoms, urine testing, and medical imaging. Blood tests may also be useful. Calculi are typically classified by their location, being referred to medically as nephrolithiasis (in the kidney), ureterolithiasis (in the ureter), or cystolithiasis (in the bladder). Calculi are also classified by what they are made of, such as from calcium oxalate, uric acid, struvite, or cystine.
In those who have had renal calculi, drinking fluids, especially water, is a way to prevent them. Drinking fluids such that more than two liters of urine are produced per day is recommended. If fluid intake alone is not effective to prevent renal calculi, the medications thiazide diuretic, citrate, or allopurinol may be suggested. Soft drinks containing phosphoric acid (typically colas) should be avoided. When a calculus causes no symptoms, no treatment is needed. For those with symptoms, pain control is usually the first measure, using medications such as nonsteroidal anti-inflammatory drugs or opioids.[needs update] Larger calculi may be helped to pass with the medication tamsulosin, or may require procedures for removal such as extracorporeal shockwave therapy (ESWT), laser lithotripsy (LL), or a percutaneous nephrolithotomy (PCNL).
Renal calculi have affected humans throughout history with a description of surgery to remove them dating from as early as 600 BC in ancient India by Sushruta. Between 1% and 15% of people globally are affected by renal calculi at some point in their lives. In 2015, 22.1 million cases occurred, resulting in about 16,100 deaths. They have become more common in the Western world since the 1970s. Generally, more men are affected than women. The prevalence and incidence of the disease rises worldwide and continues to be challenging for patients, physicians, and healthcare systems alike. In this context, epidemiological studies are striving to elucidate the worldwide changes in the patterns and the burden of the disease and identify modifiable risk factors that contribute to the development of renal calculi.
The hallmark of a stone that obstructs the ureter or renal pelvis is excruciating, intermittent pain that radiates from the flank to the groin or to the inner thigh. This is due to the transfer of referred pain signals from the lower thoracic splanchnic nerves to the lumbar splanchnic nerves as the stone passes down from the kidney or proximal ureter to the distal ureter. This pain, known as renal colic, is often described as one of the strongest pain sensations known. Renal colic caused by kidney stones is commonly accompanied by urinary urgency, restlessness, frequent urination, blood in the urine, sweating, nausea, and vomiting. It typically comes in waves lasting 20 to 60 minutes caused by peristaltic contractions of the ureter as it attempts to expel the stone.
The embryological link between the urinary tract, the genital system, and the gastrointestinal tract is the basis of the radiation of pain to the gonads, as well as the nausea and vomiting that are also common in urolithiasis. Postrenal azotemia and hydronephrosis can be observed following the obstruction of urine flow through one or both ureters.
Pain in the lower-left quadrant can sometimes be confused with diverticulitis because the sigmoid colon overlaps the ureter, and the exact location of the pain may be difficult to isolate due to the proximity of these two structures.