
Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
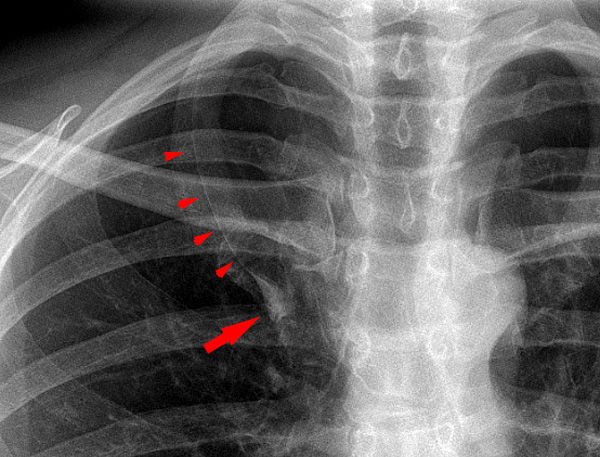
Azygos lobe
View on Wikipedia
In human anatomy, an azygos lobe is a normal anatomical variation of the upper lobe of the right lung.[1] It is seen in 0.3% of the population.[2] Embryologically, it arises from an anomalous lateral course of the azygos vein,[3] in a pleural septum within the apical segment of the right upper lobe or in other words an azygos lobe is formed when the right posterior cardinal vein, one of the precursors of the azygos vein, fails to migrate over the apex of the lung and penetrates it instead, carrying along two pleural layers as the azygous fissure, that invaginates into the upper portion of the right upper lobe.[1]
Clinical significance
[edit]An azygos lobe is usually an incidental finding on chest x-ray or CT scan. It is asymptomatic and not associated with any morbidity.[4][5] However, it can cause technical problems in thoracoscopic procedures.[6] The presence of the azygos lobe could alter the normal location of the superior vena cava or may be associated with other anomalies, including esophageal atresia or intrapulmonary right brachiocephalic veins.[7]
Additional images
[edit]

References
[edit]- ^ a b Amini B. "Azygos lobe | Radiology Reference Article | Radiopaedia.org". Radiopaedia.
- ^ Yurasakpong, Laphatrada; Yammine, Kaissar; Limpanuparb, Taweetham; Janta, Sirorat; Chaiyamoon, Arada; Kruepunga, Nutmethee; Meemon, Krai; Suwannakhan, Athikhun (2021-05-07). "The prevalence of the azygos lobe: A meta‐analysis of 1,033,083 subjects". Clinical Anatomy. 34 (6): 872–883. doi:10.1002/ca.23737. ISSN 0897-3806. PMID 33908686. S2CID 233428865.
- ^ Demos TC, Posniak HV, Pierce KL, Olson MC, Muscato M (May 2004). "Venous anomalies of the thorax". AJR. American Journal of Roentgenology. 182 (5): 1139–50. doi:10.2214/ajr.182.5.1821139. PMID 15100109.
- ^ Akhtar J, Lal A, Martin KB, Popkin J (2018-01-01). "Azygos lobe: A rare cause of right paratracheal opacity". Respiratory Medicine Case Reports. 23: 136–137. doi:10.1016/j.rmcr.2018.02.001. PMC 5925948. PMID 29719800.
- ^ Caceres J, Mata JM, Andreu J (March 1998). "The azygos lobe: normal variants that may simulate disease". European Journal of Radiology. 27 (1): 15–20. doi:10.1016/s0720-048x(97)00146-0. PMID 9587765.
- ^ Sieunarine K, May J, White GH, Harris JP (August 1997). "Anomalous azygos vein: A potential danger during endoscopic thoracic sympathectomy". Australian and New Zealand Journal of Surgery. 67 (8): 578–9. doi:10.1111/j.1445-2197.1997.tb02046.x. PMID 9287933.
- ^ Al-Mnayyis, Asma’a; Al-Alami, Zina; Altamimi, Neveen; Alawneh, Khaled Z.; Aleshawi, Abdelwahab (2020-07-10). "Azygos Lobe: Prevalence of an Anatomical Variant and Its Recognition among Postgraduate Physicians". Diagnostics. 10 (7): 470. doi:10.3390/diagnostics10070470. ISSN 2075-4418. PMC 7400486. PMID 32664403.
Further reading
[edit]- Sidhu R, Dhanadia A, Shah H, Chudasama N (May 2015). "Eluding normal variant". Lung India. 32 (3): 289–91. doi:10.4103/0970-2113.156258. PMC 4429398. PMID 25983422.
- Mata J, Cáceres J, Alegret X, Coscojuela P, De Marcos JA (May 1991). "Imaging of the azygos lobe: normal anatomy and variations" (PDF). AJR. American Journal of Roentgenology. 156 (5): 931–7. doi:10.2214/ajr.156.5.2017954. PMID 2017954.[permanent dead link]