Recent from talks
Cutaneous leishmaniasis
Knowledge base stats:
Talk channels stats:
Members stats:
Cutaneous leishmaniasis
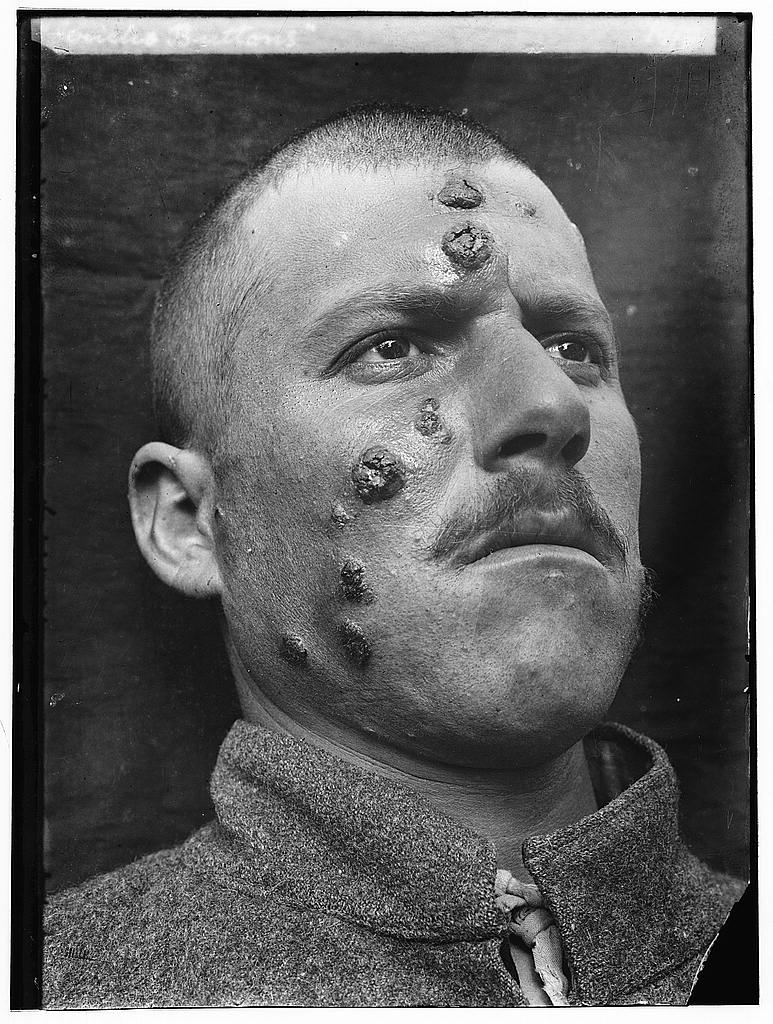
Cutaneous leishmaniasis is the most common form of leishmaniasis affecting humans. It is a skin infection caused by a single-celled parasite that is transmitted by the bite of a phlebotomine sand fly. About 30 species of Leishmania may cause cutaneous leishmaniasis. This disease is considered to be a zoonosis (an infectious disease that is naturally transmissible from animals to humans), with the exception of Leishmania tropica, which is often an anthroponotic disease (an infectious disease that is naturally transmissible from humans to vertebrate animals).
Post-kala-azar dermal leishmaniasis (PKDL) is a recurrence of kala-azar that may appear on the skin of affected individuals months and up to 20 years after being partially treated, untreated, or even in those considered adequately treated. In Sudan, they can be demonstrated in up to 60% of treated cases. They manifest as hypopigmented skin lesions (such as macules, papules, or nodules), or facial redness. Though any organism causing kala-azar can lead to PKDL, it is commonly associated with L. donovani. which gives different disease patterns in India and Sudan. In the Indian variant, nodules enlarge with time and form plaques, but rarely ulcerate, while nodules from the African variety often ulcerate as they progress. Nerve involvement is common in the African variety, but rare on the Indian subcontinent. Histology demonstrates a mixture of chronic inflammatory cells, with macrophage or epitheloid granuloma possible. Parasite concentration is not consistent among studies, perhaps reflecting low sensitivity of diagnostic methods used in earlier entries.[citation needed]
The current approach to diagnosis involves:
Newer polymerase chain reaction-based tools have higher sensitivity and specificity. Emergence of PKDL has been reported in HIV-affected individuals, and may become a problem in the future.
Sodium stibogluconate alone or in combination with rifampicin is used for the treatment of PKDL for a long course of up to 4 months. Compliance can be an issue for such a long course.[citation needed]
Mucocutaneous leishmaniasis is an especially disturbing form of cutaneous leishmaniasis, because it produces destructive and disfiguring lesions of the face. It is most often caused by L. braziliensis, but cases caused by L. aethiopica have also been described.
Mucocutaneous leishmaniasis is very difficult to treat. Treatment involves the use of pentavalent antimonial compounds, which are highly toxic (common side effects include thrombophlebitis, pancreatitis, cardiotoxicity, and hepatotoxicity) and not very effective. For example, in one study, despite treatment with high doses of sodium stibogluconate for 28 days, only 30% of patients remained disease-free at their 12-month follow-up. Even in those patients who achieve an apparent cure, as many as 19% will relapse. Several drug combinations with immunomodulators have been tested; for example, a combination of pentoxifylline (inhibitor of TNF-α) and a pentavalent antimonial at a high dose for 30 days in a small-scale (23 patients), randomised placebo-controlled study from Brazil achieved cure rates of 90% and reduced time to cure, a result that should be interpreted cautiously in light of inherent limitations of small-scale studies. In an earlier small-scale (12 patients) study, addition of imiquimod showed promising results, which need to be confirmed in larger trials.
Promastigotes of Leishmania are transmitted to human skin by the bite of a sandfly. Leishmania parasites then invade human macrophages and replicate intracellularly. A raised, red lesion develops at the site of the bite (often weeks or sometimes years afterwards). The lesion then ulcerates and may become secondarily infected with bacteria. In many species (for example, L. major), the lesion often spontaneously heals with atrophic scarring. In some species (for example, L. braziliensis), the lesion may spontaneously heal with scarring, but then reappear elsewhere (especially as destructive mucocutaneous lesions). Lesions of other Leishmania species may spontaneously heal and then reappear as satellite lesions around the site of the original lesion, or along the route of lymphatic drainage.[citation needed]
Hub AI
Cutaneous leishmaniasis AI simulator
(@Cutaneous leishmaniasis_simulator)
Cutaneous leishmaniasis
Cutaneous leishmaniasis is the most common form of leishmaniasis affecting humans. It is a skin infection caused by a single-celled parasite that is transmitted by the bite of a phlebotomine sand fly. About 30 species of Leishmania may cause cutaneous leishmaniasis. This disease is considered to be a zoonosis (an infectious disease that is naturally transmissible from animals to humans), with the exception of Leishmania tropica, which is often an anthroponotic disease (an infectious disease that is naturally transmissible from humans to vertebrate animals).
Post-kala-azar dermal leishmaniasis (PKDL) is a recurrence of kala-azar that may appear on the skin of affected individuals months and up to 20 years after being partially treated, untreated, or even in those considered adequately treated. In Sudan, they can be demonstrated in up to 60% of treated cases. They manifest as hypopigmented skin lesions (such as macules, papules, or nodules), or facial redness. Though any organism causing kala-azar can lead to PKDL, it is commonly associated with L. donovani. which gives different disease patterns in India and Sudan. In the Indian variant, nodules enlarge with time and form plaques, but rarely ulcerate, while nodules from the African variety often ulcerate as they progress. Nerve involvement is common in the African variety, but rare on the Indian subcontinent. Histology demonstrates a mixture of chronic inflammatory cells, with macrophage or epitheloid granuloma possible. Parasite concentration is not consistent among studies, perhaps reflecting low sensitivity of diagnostic methods used in earlier entries.[citation needed]
The current approach to diagnosis involves:
Newer polymerase chain reaction-based tools have higher sensitivity and specificity. Emergence of PKDL has been reported in HIV-affected individuals, and may become a problem in the future.
Sodium stibogluconate alone or in combination with rifampicin is used for the treatment of PKDL for a long course of up to 4 months. Compliance can be an issue for such a long course.[citation needed]
Mucocutaneous leishmaniasis is an especially disturbing form of cutaneous leishmaniasis, because it produces destructive and disfiguring lesions of the face. It is most often caused by L. braziliensis, but cases caused by L. aethiopica have also been described.
Mucocutaneous leishmaniasis is very difficult to treat. Treatment involves the use of pentavalent antimonial compounds, which are highly toxic (common side effects include thrombophlebitis, pancreatitis, cardiotoxicity, and hepatotoxicity) and not very effective. For example, in one study, despite treatment with high doses of sodium stibogluconate for 28 days, only 30% of patients remained disease-free at their 12-month follow-up. Even in those patients who achieve an apparent cure, as many as 19% will relapse. Several drug combinations with immunomodulators have been tested; for example, a combination of pentoxifylline (inhibitor of TNF-α) and a pentavalent antimonial at a high dose for 30 days in a small-scale (23 patients), randomised placebo-controlled study from Brazil achieved cure rates of 90% and reduced time to cure, a result that should be interpreted cautiously in light of inherent limitations of small-scale studies. In an earlier small-scale (12 patients) study, addition of imiquimod showed promising results, which need to be confirmed in larger trials.
Promastigotes of Leishmania are transmitted to human skin by the bite of a sandfly. Leishmania parasites then invade human macrophages and replicate intracellularly. A raised, red lesion develops at the site of the bite (often weeks or sometimes years afterwards). The lesion then ulcerates and may become secondarily infected with bacteria. In many species (for example, L. major), the lesion often spontaneously heals with atrophic scarring. In some species (for example, L. braziliensis), the lesion may spontaneously heal with scarring, but then reappear elsewhere (especially as destructive mucocutaneous lesions). Lesions of other Leishmania species may spontaneously heal and then reappear as satellite lesions around the site of the original lesion, or along the route of lymphatic drainage.[citation needed]
Recent media