
Community hub
Recent from talks
Contribute something to knowledge base
Content stats: 0 posts, 0 articles, 1 media, 0 notes
Members stats: 0 subscribers, 0 contributors, 0 moderators, 0 supporters
Subscribers
Supporters
Contributors
Moderators
Hub AI
Bronchiolitis obliterans AI simulator
(@Bronchiolitis obliterans_simulator)
Hub AI
Bronchiolitis obliterans AI simulator
(@Bronchiolitis obliterans_simulator)
Bronchiolitis obliterans
Bronchiolitis obliterans (BO), also known as obliterative bronchiolitis, constrictive bronchiolitis and popcorn lung, is a disease that results in obstruction of the smallest airways of the lungs (bronchioles) due to inflammation. Symptoms include a dry cough, shortness of breath, wheezing and feeling tired. These symptoms generally get worse over weeks to months. It is not related to cryptogenic organizing pneumonia, previously known as bronchiolitis obliterans organizing pneumonia.
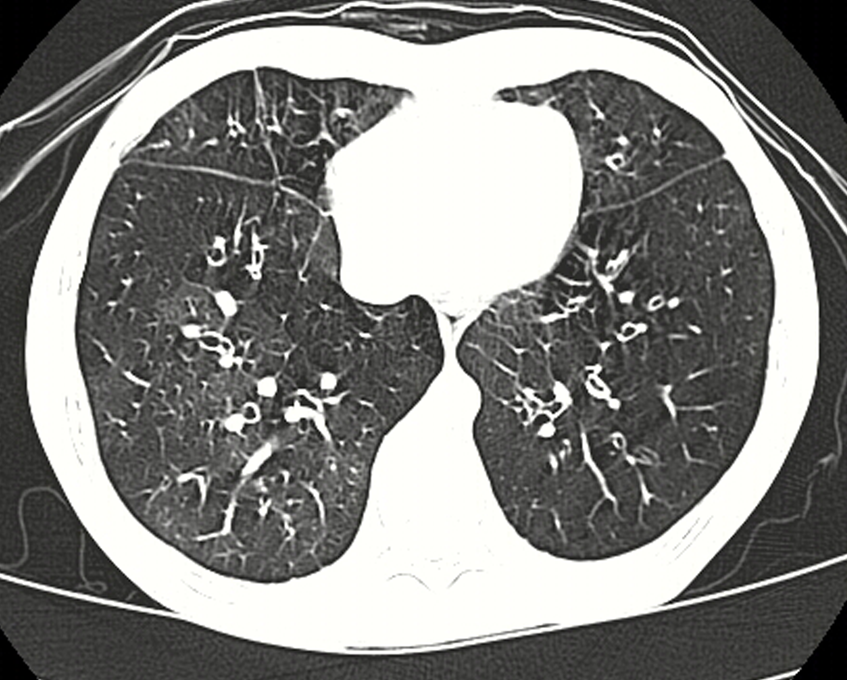
Causes include breathing in toxic fumes, respiratory infections, connective tissue disorder or complications following a bone marrow or heart-lung transplant. Symptoms may not occur until two to eight weeks following toxic exposure or infection. The underlying mechanism involves inflammation that results in scar tissue formation. Diagnosis is by CT scan, pulmonary function tests or lung biopsy. A chest X-ray is often normal.
While the disease is not reversible, treatments can slow further worsening. This may include the use of corticosteroids or immunosuppressive medication. A lung transplant may be offered. Outcomes are often poor, with most people dying in months to years.
Bronchiolitis obliterans is rare in the general population. It, however, affects about 75% of people by ten years following a lung transplant and up to 10% of people who have received a bone marrow transplant from someone else. The condition was first clearly described in 1981. Prior descriptions occurred as early as 1956, with the term "bronchiolitis obliterans" used first by Reynaud in 1835.
Bronchiolitis obliterans results in worsening shortness of breath, wheezing, and a dry cough. The symptoms can start gradually, or severe symptoms can occur suddenly. These symptoms represent an obstructive pattern that is non-reversible with bronchodilator therapy, and need to be related to various lung insults. These insults include inhalation damage, post transplant auto-immune injury, post-infectious disease, drug reactions, and several auto-immune diseases.
Bronchiolitis obliterans has many possible causes, including collagen vascular disease, transplant rejection in organ transplant patients, viral infection (adenovirus, respiratory syncytial virus, influenza, HIV, cytomegalovirus), Stevens–Johnson syndrome, Pneumocystis pneumonia, drug reaction, aspiration and complications of prematurity (bronchopulmonary dysplasia), and exposure to toxic fumes. Toxins implicated in the condition include diacetyl, sulfur dioxide, nitrogen dioxide, ammonia, chlorine, thionyl chloride, methyl isocyanate, hydrogen fluoride, hydrogen bromide, hydrogen chloride, hydrogen sulfide, phosgene, polyamide-amine dyes, mustard gas and ozone. It can also be present in patients with IBD, systemic lupus erythematosus, juvenile idiopathic arthritis, rheumatoid arthritis, GERD, IgA nephropathy, and ataxia telangiectasia. Activated charcoal has been known to cause it when aspirated. The ingestion of large doses of papaverine in the vegetable Sauropus androgynus has caused it. Additionally, the disorder may be idiopathic (without known cause).
Bronchiolitis obliterans is a common complication in lung transplants because transplanted lungs are at greater risk of alloimmunization as compared to healthy lungs. The disease is often termed bronchiolitis obliterans syndrome (BOS) in the setting of post lung transplantation and hematopoietic stem cell transplant (HSCT). Patients who develop BOS post lung transplant vary in disease latency and severity. Patients often initially have normal lung function on pulmonary function testing and have normal chest radiographs. As the disease progresses they begin to have symptoms of shortness of breath, cough, and wheezing as their lung function declines. The Journal of Heart and Lung Transplantation published updated guidelines in 2001 for grading the severity of BOS. The original guidelines and classification system were published in 1993 by the International Society for Heart and Lung Transplantation. Their scoring system is based on the changes in FEV1 in patients from their baseline. When patients are first diagnosed with BOS they have their baseline lung function established by doing pulmonary function testing at the time of diagnosis. The BOS scoring system is as follows:
BOS 0: FEV1 > 90% of baseline and FEF25-75 > 75% of baseline
Bronchiolitis obliterans
Bronchiolitis obliterans (BO), also known as obliterative bronchiolitis, constrictive bronchiolitis and popcorn lung, is a disease that results in obstruction of the smallest airways of the lungs (bronchioles) due to inflammation. Symptoms include a dry cough, shortness of breath, wheezing and feeling tired. These symptoms generally get worse over weeks to months. It is not related to cryptogenic organizing pneumonia, previously known as bronchiolitis obliterans organizing pneumonia.
Causes include breathing in toxic fumes, respiratory infections, connective tissue disorder or complications following a bone marrow or heart-lung transplant. Symptoms may not occur until two to eight weeks following toxic exposure or infection. The underlying mechanism involves inflammation that results in scar tissue formation. Diagnosis is by CT scan, pulmonary function tests or lung biopsy. A chest X-ray is often normal.
While the disease is not reversible, treatments can slow further worsening. This may include the use of corticosteroids or immunosuppressive medication. A lung transplant may be offered. Outcomes are often poor, with most people dying in months to years.
Bronchiolitis obliterans is rare in the general population. It, however, affects about 75% of people by ten years following a lung transplant and up to 10% of people who have received a bone marrow transplant from someone else. The condition was first clearly described in 1981. Prior descriptions occurred as early as 1956, with the term "bronchiolitis obliterans" used first by Reynaud in 1835.
Bronchiolitis obliterans results in worsening shortness of breath, wheezing, and a dry cough. The symptoms can start gradually, or severe symptoms can occur suddenly. These symptoms represent an obstructive pattern that is non-reversible with bronchodilator therapy, and need to be related to various lung insults. These insults include inhalation damage, post transplant auto-immune injury, post-infectious disease, drug reactions, and several auto-immune diseases.
Bronchiolitis obliterans has many possible causes, including collagen vascular disease, transplant rejection in organ transplant patients, viral infection (adenovirus, respiratory syncytial virus, influenza, HIV, cytomegalovirus), Stevens–Johnson syndrome, Pneumocystis pneumonia, drug reaction, aspiration and complications of prematurity (bronchopulmonary dysplasia), and exposure to toxic fumes. Toxins implicated in the condition include diacetyl, sulfur dioxide, nitrogen dioxide, ammonia, chlorine, thionyl chloride, methyl isocyanate, hydrogen fluoride, hydrogen bromide, hydrogen chloride, hydrogen sulfide, phosgene, polyamide-amine dyes, mustard gas and ozone. It can also be present in patients with IBD, systemic lupus erythematosus, juvenile idiopathic arthritis, rheumatoid arthritis, GERD, IgA nephropathy, and ataxia telangiectasia. Activated charcoal has been known to cause it when aspirated. The ingestion of large doses of papaverine in the vegetable Sauropus androgynus has caused it. Additionally, the disorder may be idiopathic (without known cause).
Bronchiolitis obliterans is a common complication in lung transplants because transplanted lungs are at greater risk of alloimmunization as compared to healthy lungs. The disease is often termed bronchiolitis obliterans syndrome (BOS) in the setting of post lung transplantation and hematopoietic stem cell transplant (HSCT). Patients who develop BOS post lung transplant vary in disease latency and severity. Patients often initially have normal lung function on pulmonary function testing and have normal chest radiographs. As the disease progresses they begin to have symptoms of shortness of breath, cough, and wheezing as their lung function declines. The Journal of Heart and Lung Transplantation published updated guidelines in 2001 for grading the severity of BOS. The original guidelines and classification system were published in 1993 by the International Society for Heart and Lung Transplantation. Their scoring system is based on the changes in FEV1 in patients from their baseline. When patients are first diagnosed with BOS they have their baseline lung function established by doing pulmonary function testing at the time of diagnosis. The BOS scoring system is as follows:
BOS 0: FEV1 > 90% of baseline and FEF25-75 > 75% of baseline
Recent media
Recent media