Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
5-HT1A receptor
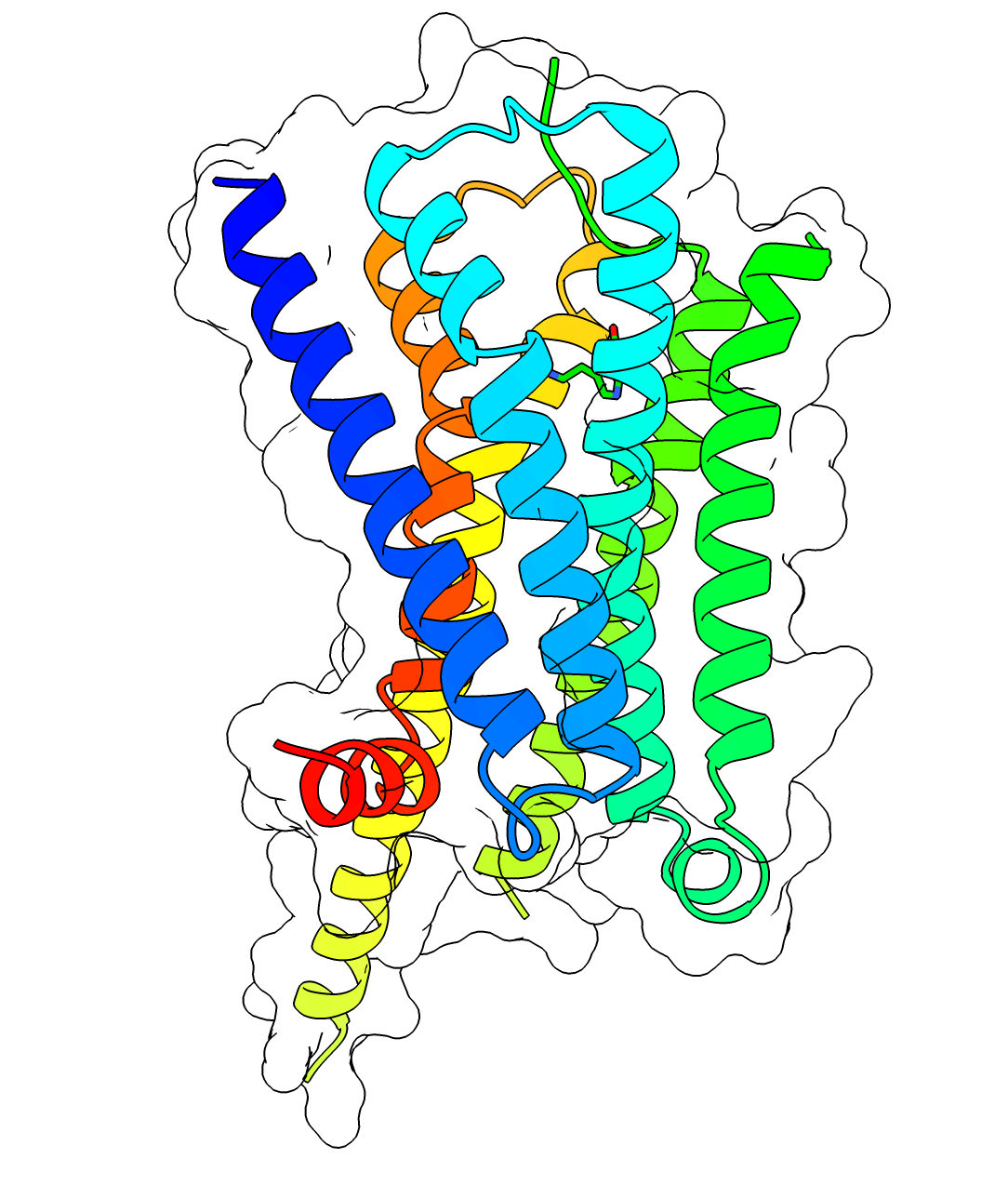
The serotonin 1A receptor (or 5-HT1A receptor) is a subtype of serotonin receptors, or 5-HT receptors, that binds serotonin, also known as 5-HT, a neurotransmitter. 5-HT1A is expressed in the brain, spleen, and neonatal kidney. It is a G protein-coupled receptor (GPCR), coupled to the Gi protein, and its activation in the brain mediates hyperpolarization and reduction of firing rate of the postsynaptic neuron. In humans, the serotonin 1A receptor is encoded by the HTR1A gene.
The 5-HT1A receptor is the most widespread of all the 5-HT receptors. In the central nervous system, 5-HT1A receptors exist in the cerebral cortex, hippocampus, septum, amygdala, and raphe nucleus in high densities, while low amounts also exist in the basal ganglia and thalamus. The 5-HT1A receptors in the raphe nucleus are largely somatodendritic autoreceptors, whereas those in other areas such as the hippocampus are postsynaptic receptors.
5-HT1A receptor agonists are involved in neuromodulation. They decrease blood pressure and heart rate via a central mechanism, by inducing peripheral vasodilation, and by stimulating the vagus nerve. These effects are the result of activation of 5-HT1A receptors within the rostral ventrolateral medulla. The sympatholytic antihypertensive drug urapidil is an α1-adrenergic receptor antagonist and 5-HT1A receptor agonist, and it has been demonstrated that the latter property contributes to its overall therapeutic effects. Vasodilation of the blood vessels in the skin via central 5-HT1A activation increases heat dissipation from the organism out into the environment, causing a decrease in body temperature.
Activation of central 5-HT1A receptors triggers the release or inhibition of norepinephrine depending on species, presumably from the locus coeruleus, which then reduces or increases neuronal tone to the iris sphincter muscle by modulation of postsynaptic α2-adrenergic receptors within the Edinger-Westphal nucleus, resulting in pupil dilation in rodents, and pupil constriction in primates including humans.
5-HT1A receptor agonists like buspirone and flesinoxan show efficacy in relieving anxiety and depression. Buspirone, tandospirone, and gepirone are currently approved for these indications in different parts of the world. Others such as flesinoxan, flibanserin, and naluzotan have also been investigated, though none have been fully developed and approved yet. Some of the atypical antipsychotics like lurasidone and aripiprazole are also partial agonists at the 5-HT1A receptor and are sometimes used in low doses as augmentations to standard antidepressants like the selective serotonin reuptake inhibitors (SSRIs). Mice lacking 5-HT1A receptors altogether (knockout) show increased anxiety but lower depressive-like behaviour.
5-HT1A autoreceptor desensitization and increased 5-HT1A receptor postsynaptic activation via general increases in serotonin levels by serotonin precursor supplementation, serotonin reuptake inhibition, or inhibition of monoamine oxidase has been shown to be a major mediator in the therapeutic benefits of most mainstream antidepressant supplements and pharmaceuticals, including serotonin precursors like L-tryptophan and 5-HTP, SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), tetracyclic antidepressants (TeCAs), and monoamine oxidase inhibitors (MAOIs). 5-HT1A receptor activation likely plays a significant role in the positive effects of serotonin releasing agents (SRAs) like MDMA (commonly known as ecstasy) as well.
5-HT1A receptors in the dorsal raphe nucleus are co-localized with neurokinin 1 (NK1) receptors and have been shown to inhibit the release of substance P, their endogenous ligand. In addition to being antidepressant and anxiolytic in effect, 5-HT1A receptor activation has also been demonstrated to be antiemetic and analgesic, and all of these properties may be mediated in part or full, depending on the property in question, by NK1 receptor inhibition. Consequently, novel NK1 receptor antagonists are now in use for the treatment of nausea and emesis, and are also being investigated for the treatment of anxiety and depression.
5-HT1A receptor activation has been shown to increase dopamine release in the medial prefrontal cortex, striatum, and hippocampus, and may be useful for improving the symptoms of schizophrenia and Parkinson's disease. As mentioned above, some of the atypical antipsychotics are 5-HT1A receptor partial agonists, and this property has been shown to enhance their clinical efficacy. Enhancement of dopamine release in these areas may also play a major role in the antidepressant and anxiolytic effects as seen upon postsynaptic activation of the 5-HT1A receptor.
Hub AI
5-HT1A receptor AI simulator
(@5-HT1A receptor_simulator)
5-HT1A receptor
The serotonin 1A receptor (or 5-HT1A receptor) is a subtype of serotonin receptors, or 5-HT receptors, that binds serotonin, also known as 5-HT, a neurotransmitter. 5-HT1A is expressed in the brain, spleen, and neonatal kidney. It is a G protein-coupled receptor (GPCR), coupled to the Gi protein, and its activation in the brain mediates hyperpolarization and reduction of firing rate of the postsynaptic neuron. In humans, the serotonin 1A receptor is encoded by the HTR1A gene.
The 5-HT1A receptor is the most widespread of all the 5-HT receptors. In the central nervous system, 5-HT1A receptors exist in the cerebral cortex, hippocampus, septum, amygdala, and raphe nucleus in high densities, while low amounts also exist in the basal ganglia and thalamus. The 5-HT1A receptors in the raphe nucleus are largely somatodendritic autoreceptors, whereas those in other areas such as the hippocampus are postsynaptic receptors.
5-HT1A receptor agonists are involved in neuromodulation. They decrease blood pressure and heart rate via a central mechanism, by inducing peripheral vasodilation, and by stimulating the vagus nerve. These effects are the result of activation of 5-HT1A receptors within the rostral ventrolateral medulla. The sympatholytic antihypertensive drug urapidil is an α1-adrenergic receptor antagonist and 5-HT1A receptor agonist, and it has been demonstrated that the latter property contributes to its overall therapeutic effects. Vasodilation of the blood vessels in the skin via central 5-HT1A activation increases heat dissipation from the organism out into the environment, causing a decrease in body temperature.
Activation of central 5-HT1A receptors triggers the release or inhibition of norepinephrine depending on species, presumably from the locus coeruleus, which then reduces or increases neuronal tone to the iris sphincter muscle by modulation of postsynaptic α2-adrenergic receptors within the Edinger-Westphal nucleus, resulting in pupil dilation in rodents, and pupil constriction in primates including humans.
5-HT1A receptor agonists like buspirone and flesinoxan show efficacy in relieving anxiety and depression. Buspirone, tandospirone, and gepirone are currently approved for these indications in different parts of the world. Others such as flesinoxan, flibanserin, and naluzotan have also been investigated, though none have been fully developed and approved yet. Some of the atypical antipsychotics like lurasidone and aripiprazole are also partial agonists at the 5-HT1A receptor and are sometimes used in low doses as augmentations to standard antidepressants like the selective serotonin reuptake inhibitors (SSRIs). Mice lacking 5-HT1A receptors altogether (knockout) show increased anxiety but lower depressive-like behaviour.
5-HT1A autoreceptor desensitization and increased 5-HT1A receptor postsynaptic activation via general increases in serotonin levels by serotonin precursor supplementation, serotonin reuptake inhibition, or inhibition of monoamine oxidase has been shown to be a major mediator in the therapeutic benefits of most mainstream antidepressant supplements and pharmaceuticals, including serotonin precursors like L-tryptophan and 5-HTP, SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), tetracyclic antidepressants (TeCAs), and monoamine oxidase inhibitors (MAOIs). 5-HT1A receptor activation likely plays a significant role in the positive effects of serotonin releasing agents (SRAs) like MDMA (commonly known as ecstasy) as well.
5-HT1A receptors in the dorsal raphe nucleus are co-localized with neurokinin 1 (NK1) receptors and have been shown to inhibit the release of substance P, their endogenous ligand. In addition to being antidepressant and anxiolytic in effect, 5-HT1A receptor activation has also been demonstrated to be antiemetic and analgesic, and all of these properties may be mediated in part or full, depending on the property in question, by NK1 receptor inhibition. Consequently, novel NK1 receptor antagonists are now in use for the treatment of nausea and emesis, and are also being investigated for the treatment of anxiety and depression.
5-HT1A receptor activation has been shown to increase dopamine release in the medial prefrontal cortex, striatum, and hippocampus, and may be useful for improving the symptoms of schizophrenia and Parkinson's disease. As mentioned above, some of the atypical antipsychotics are 5-HT1A receptor partial agonists, and this property has been shown to enhance their clinical efficacy. Enhancement of dopamine release in these areas may also play a major role in the antidepressant and anxiolytic effects as seen upon postsynaptic activation of the 5-HT1A receptor.