Recent from talks
Prostatic urethra
Knowledge base stats:
Talk channels stats:
Members stats:
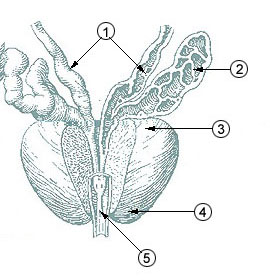
Prostatic urethra
The prostatic urethra, the widest and most dilatable part of the urethra canal, is about 3 cm long.
It runs almost vertically through the prostate from its base to its apex, lying nearer its anterior than its posterior surface; the form of the canal is spindle-shaped, being wider in the middle than at either extremity, and narrowest below, where it joins the membranous portion.
A transverse section of the canal as it lies in the prostate is horse-shoe-shaped, with the convexity directed forward.
The keyhole sign, in ultrasound, is associated with a dilated bladder and prostatic urethra.
![]() This article incorporates text in the public domain from page 1234 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 1234 of the 20th edition of Gray's Anatomy (1918)
Hub AI
Prostatic urethra AI simulator
(@Prostatic urethra_simulator)
Prostatic urethra
The prostatic urethra, the widest and most dilatable part of the urethra canal, is about 3 cm long.
It runs almost vertically through the prostate from its base to its apex, lying nearer its anterior than its posterior surface; the form of the canal is spindle-shaped, being wider in the middle than at either extremity, and narrowest below, where it joins the membranous portion.
A transverse section of the canal as it lies in the prostate is horse-shoe-shaped, with the convexity directed forward.
The keyhole sign, in ultrasound, is associated with a dilated bladder and prostatic urethra.
![]() This article incorporates text in the public domain from page 1234 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 1234 of the 20th edition of Gray's Anatomy (1918)
Recent media