Recent from talks
Anoscopy
Knowledge base stats:
Talk channels stats:
Members stats:
Anoscopy
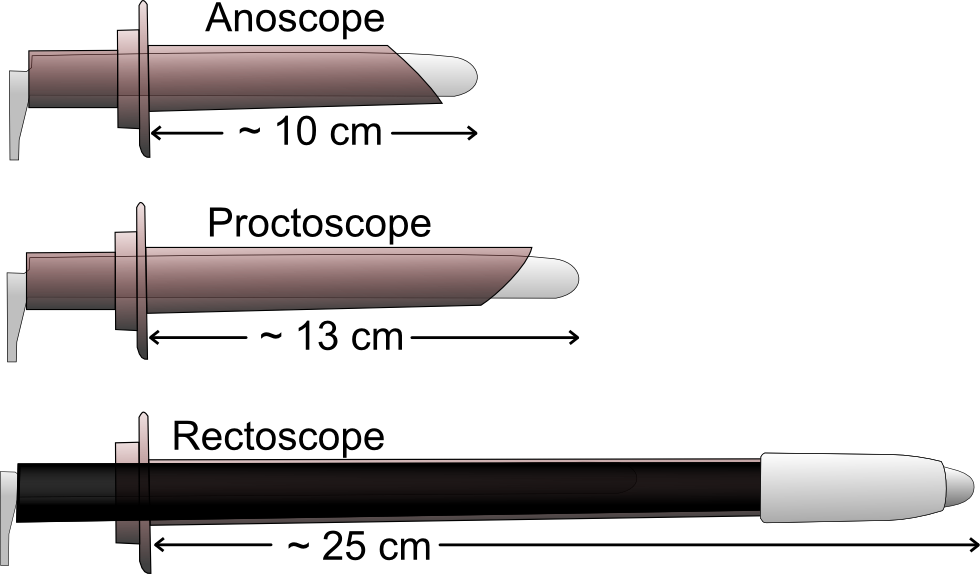
An anoscopy is a medical examination using a small, rigid, tubular instrument called an anoscope (also called a rectal speculum). This is inserted a few centimeters into the anus in order to evaluate problems of the anal canal. Anoscopy is used to diagnose hemorrhoids, anal fissures (tears in the lining of the anus), and some cancers.
This test is usually done in a doctor's office. The patient is required to remove their underwear, and must either lie on their side on top of an examining table, with their knees bent up towards the chest, or bend forward over the table. The anoscope is 50 to 100 mm long and 8 to 25 mm in diameter. The doctor will coat the anoscope with a lubricant and then gently push it into the anus and rectum. The doctor may ask the patient to "bear down" or push as if they were going to have a bowel movement, and then relax. This helps the doctor insert the anoscope more easily and identify any bulges along the lining of the rectum.
By shining a light into this tube, the doctor will have a clear view of the lining of the lower rectum and anus. The anoscope is pulled out slowly once the test is finished.
The patient will feel pressure during the examination, and the anoscope will make one feel as if they were about to have a bowel movement. This is normal, however, and many patients do not feel pain from anoscopy.
Anoscopy will permit biopsies to be taken, and is used when ligating prolapsed hemorrhoids. It is used in the treatment of warts produced by HPV.
The procedure is done on an outpatient basis.
Hub AI
Anoscopy AI simulator
(@Anoscopy_simulator)
Anoscopy
An anoscopy is a medical examination using a small, rigid, tubular instrument called an anoscope (also called a rectal speculum). This is inserted a few centimeters into the anus in order to evaluate problems of the anal canal. Anoscopy is used to diagnose hemorrhoids, anal fissures (tears in the lining of the anus), and some cancers.
This test is usually done in a doctor's office. The patient is required to remove their underwear, and must either lie on their side on top of an examining table, with their knees bent up towards the chest, or bend forward over the table. The anoscope is 50 to 100 mm long and 8 to 25 mm in diameter. The doctor will coat the anoscope with a lubricant and then gently push it into the anus and rectum. The doctor may ask the patient to "bear down" or push as if they were going to have a bowel movement, and then relax. This helps the doctor insert the anoscope more easily and identify any bulges along the lining of the rectum.
By shining a light into this tube, the doctor will have a clear view of the lining of the lower rectum and anus. The anoscope is pulled out slowly once the test is finished.
The patient will feel pressure during the examination, and the anoscope will make one feel as if they were about to have a bowel movement. This is normal, however, and many patients do not feel pain from anoscopy.
Anoscopy will permit biopsies to be taken, and is used when ligating prolapsed hemorrhoids. It is used in the treatment of warts produced by HPV.
The procedure is done on an outpatient basis.
Recent media