Recent from talks
Cholescintigraphy
Knowledge base stats:
Talk channels stats:
Members stats:
Cholescintigraphy
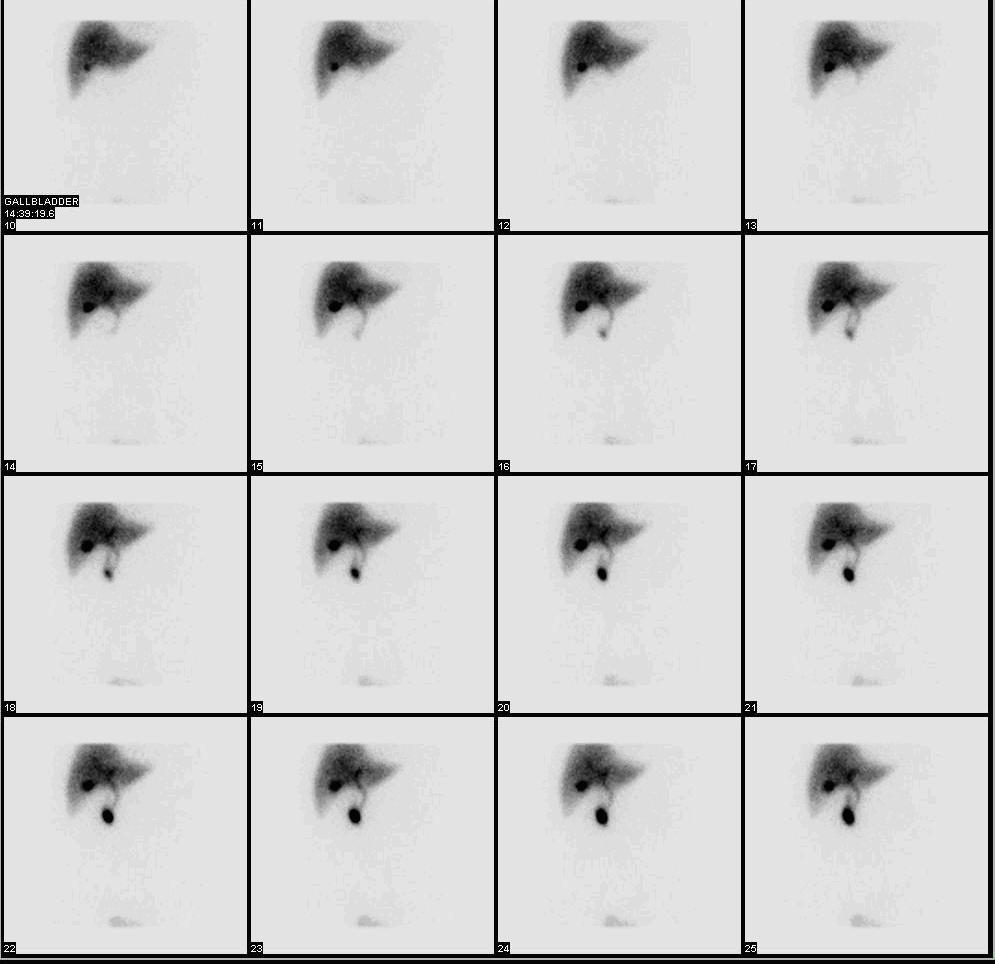
Cholescintigraphy or hepatobiliary scintigraphy is scintigraphy of the hepatobiliary tract, including the gallbladder and bile ducts. The image produced by this type of medical imaging, called a cholescintigram, is also known by other names depending on which radiotracer is used, such as HIDA scan, PIPIDA scan, DISIDA scan, or BrIDA scan. Cholescintigraphic scanning is a nuclear medicine procedure to evaluate the health and function of the gallbladder and biliary system. A radioactive tracer is injected through any accessible vein and then allowed to circulate to the liver, where it is excreted into the bile ducts and stored by the gallbladder until released into the duodenum.
Use of cholescintigraphic scans as a first-line form of imaging varies depending on indication. For example for cholecystitis, cheaper and less invasive ultrasound imaging may be preferred, while for bile reflux cholescintigraphy may be the first choice.
The word cholescintigraphy (/ˌkoʊliˌsɪnˈtɪɡrəfi/) uses combining forms of chole- + scinti(llation) + -graphy, most literally "bile + flash + recording".
In the absence of gallbladder disease, the gallbladder is visualized within 1 hour of the injection of the radioactive tracer.[citation needed]
If the gallbladder is not visualized within 4 hours after the injection, this indicates either cholecystitis or cystic duct obstruction, such as by cholelithiasis (gallstone formation).
The investigation is usually conducted after an ultrasonographic examination of the abdominal right upper quadrant for a patient presenting with abdominal pain. If the noninvasive ultrasound examination fails to demonstrate gallstones, or other obstruction to the gallbladder or biliary tree, in an attempt to establish a cause of right upper quadrant pain, a cholescintigraphic scan can be performed as a more sensitive and specific test.[citation needed]
Cholescintigraphy for acute cholecystitis has sensitivity of 97%, specificity of 94%. Several investigators have found the sensitivity being consistently higher than 90% though specificity has varied from 73–99%, yet compared to ultrasonography, cholescintigraphy has proven to be superior. The scan is also important to differentiate between neonatal hepatitis and biliary atresia, because an early surgical intervention in form of Kasai portoenterostomy or hepatoportoenterostomy can save the life of the baby as the chance of a successful operation after 3 months seriously decreases.
Cholescintigraphy is also used in diagnosis of the biliary dyskinesia.
Hub AI
Cholescintigraphy AI simulator
(@Cholescintigraphy_simulator)
Cholescintigraphy
Cholescintigraphy or hepatobiliary scintigraphy is scintigraphy of the hepatobiliary tract, including the gallbladder and bile ducts. The image produced by this type of medical imaging, called a cholescintigram, is also known by other names depending on which radiotracer is used, such as HIDA scan, PIPIDA scan, DISIDA scan, or BrIDA scan. Cholescintigraphic scanning is a nuclear medicine procedure to evaluate the health and function of the gallbladder and biliary system. A radioactive tracer is injected through any accessible vein and then allowed to circulate to the liver, where it is excreted into the bile ducts and stored by the gallbladder until released into the duodenum.
Use of cholescintigraphic scans as a first-line form of imaging varies depending on indication. For example for cholecystitis, cheaper and less invasive ultrasound imaging may be preferred, while for bile reflux cholescintigraphy may be the first choice.
The word cholescintigraphy (/ˌkoʊliˌsɪnˈtɪɡrəfi/) uses combining forms of chole- + scinti(llation) + -graphy, most literally "bile + flash + recording".
In the absence of gallbladder disease, the gallbladder is visualized within 1 hour of the injection of the radioactive tracer.[citation needed]
If the gallbladder is not visualized within 4 hours after the injection, this indicates either cholecystitis or cystic duct obstruction, such as by cholelithiasis (gallstone formation).
The investigation is usually conducted after an ultrasonographic examination of the abdominal right upper quadrant for a patient presenting with abdominal pain. If the noninvasive ultrasound examination fails to demonstrate gallstones, or other obstruction to the gallbladder or biliary tree, in an attempt to establish a cause of right upper quadrant pain, a cholescintigraphic scan can be performed as a more sensitive and specific test.[citation needed]
Cholescintigraphy for acute cholecystitis has sensitivity of 97%, specificity of 94%. Several investigators have found the sensitivity being consistently higher than 90% though specificity has varied from 73–99%, yet compared to ultrasonography, cholescintigraphy has proven to be superior. The scan is also important to differentiate between neonatal hepatitis and biliary atresia, because an early surgical intervention in form of Kasai portoenterostomy or hepatoportoenterostomy can save the life of the baby as the chance of a successful operation after 3 months seriously decreases.
Cholescintigraphy is also used in diagnosis of the biliary dyskinesia.
Recent media