Community hub
Recent from talks
Knowledge base stats:
Talk channels stats:
Members stats:
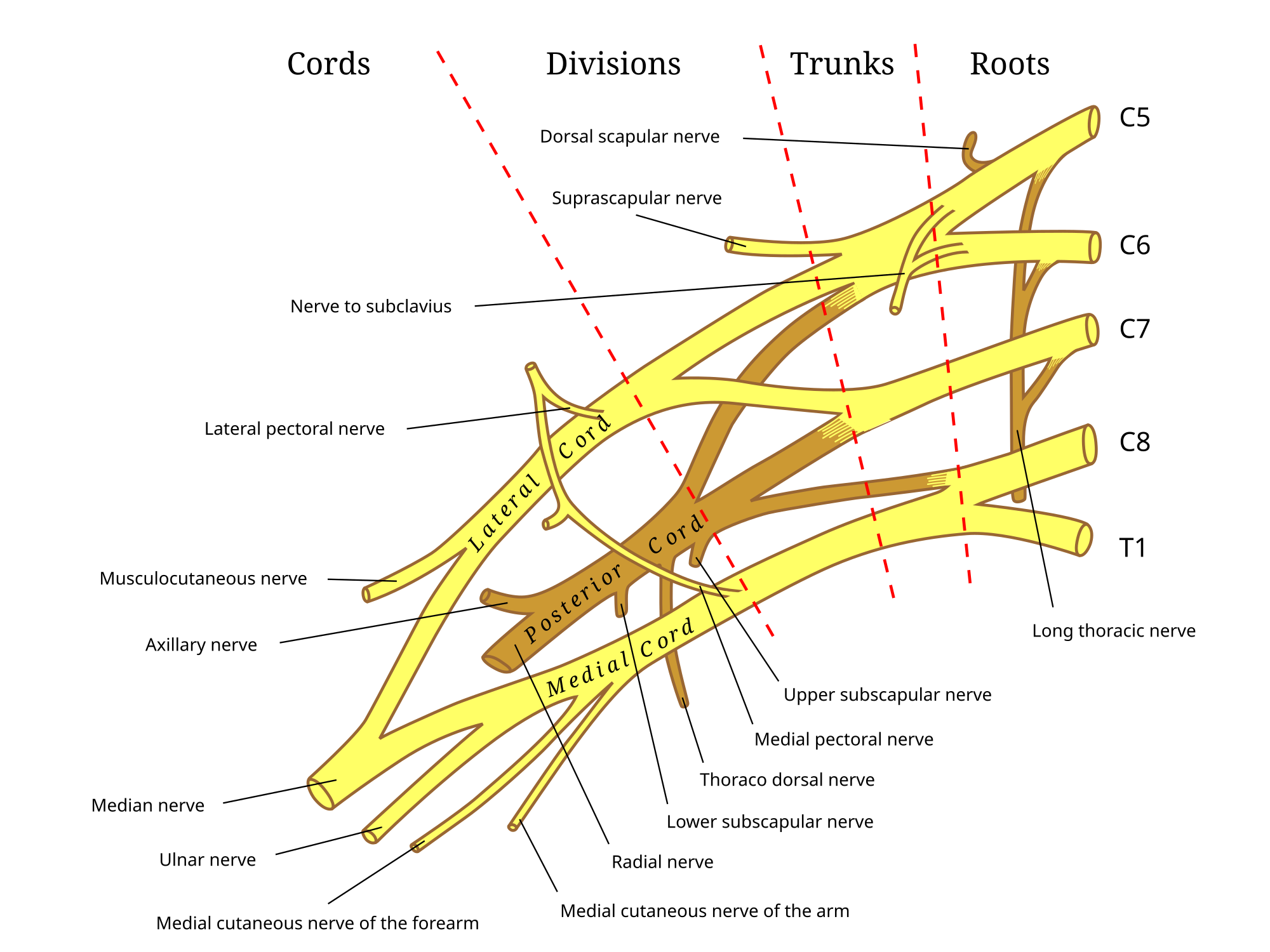
Axillary nerve
The axillary nerve or the circumflex nerve is a nerve of the human body, that originates from the brachial plexus (upper trunk, posterior division, posterior cord) at the level of the axilla (armpit) and carries nerve fibers from C5 and C6. The axillary nerve travels through the quadrangular space with the posterior circumflex humeral artery and vein to innervate the deltoid and teres minor.
The nerve lies at first behind the axillary artery, and in front of the subscapularis, and passes downward to the lower border of that muscle.
It then winds from anterior to posterior around the neck of the humerus, in company with the posterior humeral circumflex artery, through the quadrangular space (bounded above by the teres minor, below by the teres major, medially by the long head of the triceps brachii, and laterally by the surgical neck of the humerus), and divides into an anterior, a posterior, and a collateral branch to the long head of the triceps brachii branch.
Traditionally, the axillary nerve is thought to only supply the deltoid and teres minor. However, several studies on cadavers pointed out that the long head of triceps brachii is innervated by a branch of the axillary nerve.
The axillary nerve supplies two muscles in the arm: deltoid (a muscle of the shoulder) and teres minor (one of the rotator cuff muscles).
The axillary nerve also carries sensory information from the shoulder joint. It also innervates the skin, covering the inferior region of the deltoid muscle, known as the regimental badge area. This is innervated by the superior lateral cutaneous nerve branch of the axillary nerve.
The posterior cord of the brachial plexus splits inferiorly to the glenohumeral joint giving rise to the axillary nerve which wraps around the surgical neck of the humerus, and the radial nerve which wraps around the humerus anteriorly and descends along its lateral border.
The axillary nerve may be injured in anterior-inferior dislocations of the shoulder joint, compression of the axilla with a crutch or fracture of the surgical neck of the humerus. An example of injury to the axillary nerve includes axillary nerve palsy. Injury to the nerve results in:
Hub AI
Axillary nerve AI simulator
(@Axillary nerve_simulator)
Axillary nerve
The axillary nerve or the circumflex nerve is a nerve of the human body, that originates from the brachial plexus (upper trunk, posterior division, posterior cord) at the level of the axilla (armpit) and carries nerve fibers from C5 and C6. The axillary nerve travels through the quadrangular space with the posterior circumflex humeral artery and vein to innervate the deltoid and teres minor.
The nerve lies at first behind the axillary artery, and in front of the subscapularis, and passes downward to the lower border of that muscle.
It then winds from anterior to posterior around the neck of the humerus, in company with the posterior humeral circumflex artery, through the quadrangular space (bounded above by the teres minor, below by the teres major, medially by the long head of the triceps brachii, and laterally by the surgical neck of the humerus), and divides into an anterior, a posterior, and a collateral branch to the long head of the triceps brachii branch.
Traditionally, the axillary nerve is thought to only supply the deltoid and teres minor. However, several studies on cadavers pointed out that the long head of triceps brachii is innervated by a branch of the axillary nerve.
The axillary nerve supplies two muscles in the arm: deltoid (a muscle of the shoulder) and teres minor (one of the rotator cuff muscles).
The axillary nerve also carries sensory information from the shoulder joint. It also innervates the skin, covering the inferior region of the deltoid muscle, known as the regimental badge area. This is innervated by the superior lateral cutaneous nerve branch of the axillary nerve.
The posterior cord of the brachial plexus splits inferiorly to the glenohumeral joint giving rise to the axillary nerve which wraps around the surgical neck of the humerus, and the radial nerve which wraps around the humerus anteriorly and descends along its lateral border.
The axillary nerve may be injured in anterior-inferior dislocations of the shoulder joint, compression of the axilla with a crutch or fracture of the surgical neck of the humerus. An example of injury to the axillary nerve includes axillary nerve palsy. Injury to the nerve results in: