Recent from talks
HLA-DQ
Knowledge base stats:
Talk channels stats:
Members stats:
HLA-DQ
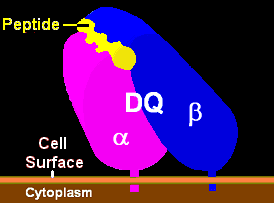
HLA-DQ (DQ) is a cell surface receptor protein found on antigen-presenting cells. It is an αβ heterodimer of type MHC class II. The α and β chains are encoded by two loci, HLA-DQA1 and HLA-DQB1, that are adjacent to each other on chromosome band 6p21.3. Both α-chain and β-chain vary greatly. A person often produces two α-chain and two β-chain variants and thus 4 isoforms of DQ. The DQ loci are in close genetic linkage to HLA-DR, and less closely linked to HLA-DP, HLA-A, HLA-B and HLA-C.
Different isoforms of DQ can bind to and present different antigens to T-cells. In this process T-cells are stimulated to grow and can signal B-cells to produce antibodies. DQ functions in recognizing and presenting foreign antigens (proteins derived from potential pathogens). But DQ is also involved in recognizing common self-antigens and presenting those antigens to the immune system in order to develop tolerance from a very young age.
When tolerance to self proteins is lost, DQ may become involved in autoimmune disease. Two autoimmune diseases in which HLA-DQ is involved are coeliac disease and type 1 diabetes. DQ mediates autoimmunity by skewing the T-cell receptor (TCR) repertoire during thymic selection. Carriers of risk serotypes such as DQ8 have a higher proportion of circulating T-cell receptors that may bind insulin, the primary autoantigen in type 1 diabetes.
DQ is one of several antigens involved in rejection of organ transplants. As a variable cell surface receptor on immune cells, these D antigens, originally HL-A4 antigens, are involved in graft-versus-host disease when lymphoid tissues are transplanted between people. Serological studies of DQ recognized that antibodies to DQ bind primarily to the β-chain. The currently used serotypes are HLA-DQ2, -DQ3, -DQ4, -DQ5, -DQ6, -DQ7, -DQ8, -DQ9. HLA-DQ1 is a weak reaction to the α-chain and was replaced by DQ5 and DQ6 serology. Serotyping is capable of identifying most aspects of DQ isoform structure and function, however sequence specific PCR is now the preferred method of determining HLA-DQA1 and HLA-DQB1 alleles, as serotyping cannot resolve, often, the critical contribution of the DQ α-chain. This can be compensated for by examining DR serotypes as well as DQ serotypes.
The name 'HLA DQ' originally describes a transplantation antigen of MHC class II category of the major histocompatibility complex of humans; however, this status is an artifact of the early era of organ transplantation.
HLA DQ functions as a cell surface receptor for foreign or self antigens. The immune system surveys antigens for foreign pathogens when presented by MHC receptors (like HLA DQ). The MHC Class II antigens are found on antigen presenting cells (APC) (macrophages, dendritic cells, and B-lymphocytes). Normally, these APC 'present' class II receptor/antigens to a great many T-cells, each with unique T-cell receptor (TCR) variants. A few TCR variants that recognize these DQ/antigen complexes are on CD4 positive (CD4+) T-cells. These T-cells, called T-helper cells, can promote the amplification of B-cells which, in turn recognize a different portion of the same antigen. Alternatively, macrophages and other megalocytes consume cells by apoptotic signaling and present self-antigens. Self antigens, in the right context, form a regulatory T-cell population that protects self tissues from immune attack or autoimmunity.
HLA-DQ (DQ) is encoded on the HLA region of chromosome 6p21.3, in what was classically known as the "D" antigen region. This region encoded the subunits for DP,-Q and -R which are the major MHC class II antigens in humans. Each of these proteins have slightly different functions and are regulated in slightly different ways.
DQ is made up of two different subunits to form an αβ-heterodimer. Each subunit is encoded by its own "gene" (a coding locus). The DQ α subunit is encoded by the HLA-DQA1 gene and the DQ β subunit is encoded by the HLA-DQB1 gene. Both loci are variable in the human population (see regional evolution).
Hub AI
HLA-DQ AI simulator
(@HLA-DQ_simulator)
HLA-DQ
HLA-DQ (DQ) is a cell surface receptor protein found on antigen-presenting cells. It is an αβ heterodimer of type MHC class II. The α and β chains are encoded by two loci, HLA-DQA1 and HLA-DQB1, that are adjacent to each other on chromosome band 6p21.3. Both α-chain and β-chain vary greatly. A person often produces two α-chain and two β-chain variants and thus 4 isoforms of DQ. The DQ loci are in close genetic linkage to HLA-DR, and less closely linked to HLA-DP, HLA-A, HLA-B and HLA-C.
Different isoforms of DQ can bind to and present different antigens to T-cells. In this process T-cells are stimulated to grow and can signal B-cells to produce antibodies. DQ functions in recognizing and presenting foreign antigens (proteins derived from potential pathogens). But DQ is also involved in recognizing common self-antigens and presenting those antigens to the immune system in order to develop tolerance from a very young age.
When tolerance to self proteins is lost, DQ may become involved in autoimmune disease. Two autoimmune diseases in which HLA-DQ is involved are coeliac disease and type 1 diabetes. DQ mediates autoimmunity by skewing the T-cell receptor (TCR) repertoire during thymic selection. Carriers of risk serotypes such as DQ8 have a higher proportion of circulating T-cell receptors that may bind insulin, the primary autoantigen in type 1 diabetes.
DQ is one of several antigens involved in rejection of organ transplants. As a variable cell surface receptor on immune cells, these D antigens, originally HL-A4 antigens, are involved in graft-versus-host disease when lymphoid tissues are transplanted between people. Serological studies of DQ recognized that antibodies to DQ bind primarily to the β-chain. The currently used serotypes are HLA-DQ2, -DQ3, -DQ4, -DQ5, -DQ6, -DQ7, -DQ8, -DQ9. HLA-DQ1 is a weak reaction to the α-chain and was replaced by DQ5 and DQ6 serology. Serotyping is capable of identifying most aspects of DQ isoform structure and function, however sequence specific PCR is now the preferred method of determining HLA-DQA1 and HLA-DQB1 alleles, as serotyping cannot resolve, often, the critical contribution of the DQ α-chain. This can be compensated for by examining DR serotypes as well as DQ serotypes.
The name 'HLA DQ' originally describes a transplantation antigen of MHC class II category of the major histocompatibility complex of humans; however, this status is an artifact of the early era of organ transplantation.
HLA DQ functions as a cell surface receptor for foreign or self antigens. The immune system surveys antigens for foreign pathogens when presented by MHC receptors (like HLA DQ). The MHC Class II antigens are found on antigen presenting cells (APC) (macrophages, dendritic cells, and B-lymphocytes). Normally, these APC 'present' class II receptor/antigens to a great many T-cells, each with unique T-cell receptor (TCR) variants. A few TCR variants that recognize these DQ/antigen complexes are on CD4 positive (CD4+) T-cells. These T-cells, called T-helper cells, can promote the amplification of B-cells which, in turn recognize a different portion of the same antigen. Alternatively, macrophages and other megalocytes consume cells by apoptotic signaling and present self-antigens. Self antigens, in the right context, form a regulatory T-cell population that protects self tissues from immune attack or autoimmunity.
HLA-DQ (DQ) is encoded on the HLA region of chromosome 6p21.3, in what was classically known as the "D" antigen region. This region encoded the subunits for DP,-Q and -R which are the major MHC class II antigens in humans. Each of these proteins have slightly different functions and are regulated in slightly different ways.
DQ is made up of two different subunits to form an αβ-heterodimer. Each subunit is encoded by its own "gene" (a coding locus). The DQ α subunit is encoded by the HLA-DQA1 gene and the DQ β subunit is encoded by the HLA-DQB1 gene. Both loci are variable in the human population (see regional evolution).
Recent media