Vermilion border
View on Wikipedia| Vermilion border | |
|---|---|
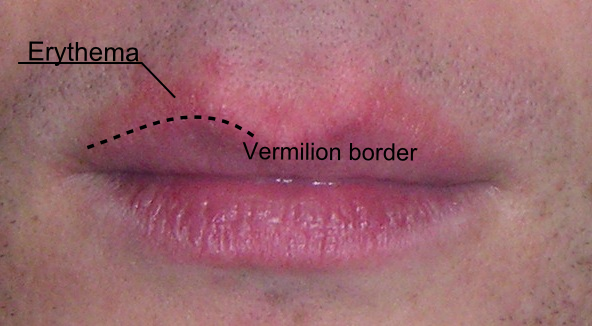
 Human lips with the vermilion border outlined. A patch of erythema above the upper lip makes it more difficult to distinguish the vermilion border. | |
| Details | |
| Identifiers | |
| Latin | pars intermedia labiorum oris |
| TH | H3.04.01.0.00010 |
| Anatomical terminology | |
The vermilion border (sometimes spelled vermillion border), also called margin or zone, is the normally sharp demarcation between the lip and the adjacent normal skin. It represents the change in the epidermis from highly keratinized external skin to less keratinized internal skin. It has no sebaceous glands, sweat glands, or facial hair.[1][2]
It has a prominence on the face, creating a focus for cosmetics (it is where lipstick is sometimes applied) and is also a location for several skin diseases. Its functional properties, however, remain unknown.[3]
Structure
[edit]The lips are composed wholly of soft tissue. The skin of the face is thicker than the skin overlying the lips where blood vessels are closer to the surface. As a consequence, the margin of the lips shows a transition between the thicker and thinner skin, represented by the vermilion border. It therefore has the appearance of a sharp line between the coloured edge of the lip and adjoining skin.[4]
It has been described as a pale, white rolled border and also as being a red line.[1][5]
This fine line of pale skin accentuates the colour difference between the vermilion and normal skin. Along the upper lip, two adjacent elevations of the vermilion border form the Cupid's bow.[6]
Microanatomy
[edit]The vermilion border represents the change in the epidermis from highly keratinized external skin to less keratinized internal skin. It has no sebaceous glands, sweat glands, or facial hair.[2][1]
There are two reasons that the border appears red in some people:
- The epithelium is thin and therefore the blood vessels are closer to the surface.[7]
- This epithelium contains eleidin which is transparent and the blood vessels are near the surface of the papillary layer, revealing the "red blood cell" color. At the angles of the mouth, there are sebaceous glands, without hair follicles, which are called Fordyce spots.[2][8]

Clinical significance
[edit]The vermilion border is important in dentistry and oral pathology as a marker to detect disease, such as in actinic cheilitis.[9]
Associated diseases
[edit]- Perioral dermatitis is a rash typically around the mouth, that spares the vermilion border.[10]
- Cheilitis glandularis may present with a burning sensation over the vermilion border. This chronic progressive condition is associated with thinning of the skin of the lips and ulceration.[11]
- Infections may involve the vermilion border. Cold sores are one common infection.[12] Impetigo is another.[13]
- Skin cancer can also occur at the vermilion border.[9]
- Fetal alcohol syndrome causes facial abnormalities which include a thin vermilion border with a smooth philtrum.[14]
Cosmetic appearance
[edit]- Sunlight exposure can blur the junction between the vermilion border and the skin. Applying lip balm and sunscreen moisturizer protects it from sunlight.[15]
Surgery
[edit]A vermilionectomy (sometimes spelled vermillionectomy) is the surgical removal of the vermilion border. It is sometimes performed to treat carcinoma of the lip.[16]
Close attention is given when repairing any injury to the vermilion border. Even 1 mm of vermilion misalignment could be noticeable.[5]
See also
[edit]References
[edit]- ^ a b c Scheid, Rickne C.; Woelfel, Julian B. (2007). "2. Oral examination: normal anatomy of the oral cavity". Woelfel's Dental Anatomy: Its Relevance to Dentistry (7th ed.). Lippincott Williams & Wilkins. pp. 81–82. ISBN 9780781768603.
- ^ a b c Chiego, Daniel J. (2018). "14. Oral mucosa". Essentials of Oral Histology and Embryology: A Clinical Approach. Elsevier. p. 170. ISBN 9780323569323.
- ^ Kobayashi, H; Tagami, H (March 2004). "Functional properties of the surface of the vermilion border of the lips are distinct from those of the facial skin". British Journal of Dermatology. 150 (3): 563–567. doi:10.1046/j.1365-2133.2003.05741.x. PMID 15030342. S2CID 42980307.
- ^ "Anatomy of the ageing lip". ENT & Audiology News. Retrieved 2018-02-04.
- ^ a b "Complex Lip Laceration: Overview, Indications, Contraindications". 2017-03-09.
{{cite journal}}: Cite journal requires|journal=(help) - ^ Luthra, Amit (2015). "Shaping Lips with Fillers". Journal of Cutaneous and Aesthetic Surgery. 8 (3): 139–142. doi:10.4103/0974-2077.167269. PMC 4645142. PMID 26644736.
- ^ Drake, Richard; Vogl, A. Wayne; Mitchell, Adam W. M. (2009-04-04). Gray's Anatomy for Students E-Book. Elsevier Health Sciences. p. 1055. ISBN 978-1437720556.
- ^ James, William D.; Berger, Timothy; Elston, Dirk (2015-04-12). Andrews' Diseases of the Skin: Clinical Dermatology. Elsevier Health Sciences. p. 793. ISBN 9780323319690.
- ^ a b Thun, Michael; Linet, Martha S.; Cerhan, James R.; Haiman, Christopher A.; Schottenfeld, David (2017-11-07). Cancer Epidemiology and Prevention. Oxford University Press. ISBN 9780190238681.
- ^ M.D., Ilya Petrou (2006-07-29). "Perioral dermatitis: It's not every rash that appears around the mouth". Dermatology Times. Retrieved 2018-02-05.
- ^ "Cheilitis Glandularis Clinical Presentation: History, Physical, Causes". emedicine.medscape.com. Retrieved 2018-02-05.
- ^ Kradin, Richard L. (2010-02-02). Diagnostic Pathology of Infectious Disease E-Book. Elsevier Health Sciences. ISBN 978-1455705986.
- ^ Eversole, Lewis R. (2011). Clinical Outline of Oral Pathology: Diagnosis and Treatment. PMPH-USA. ISBN 9781607950158.
- ^ Chudley AE, Conry J, Cook JL, Loock C, Rosales T, LeBlanc N (March 2005). "Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis". CMAJ. 172 (5 Suppl): S1 – S21. doi:10.1503/cmaj.1040302. PMC 557121. PMID 15738468.
- ^ Saucer, Caroline; Torg, Elisabeth (1996). The Female Body: An Owner's Manual : a Head-to-toe Guide to Good Health and Body Care-- at Any Age. Rodale Press. ISBN 9780875964003.
lip liner vermilion.
- ^ Rodriguez, Eduardo D.; Losee, Joseph E.; Neligan, Peter C. (2017-08-10). Plastic Surgery E-Book: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic Surgery. Elsevier Health Sciences. p. 309. ISBN 9780323356992.