Recent from talks
Gums
Knowledge base stats:
Talk channels stats:
Members stats:
Gums
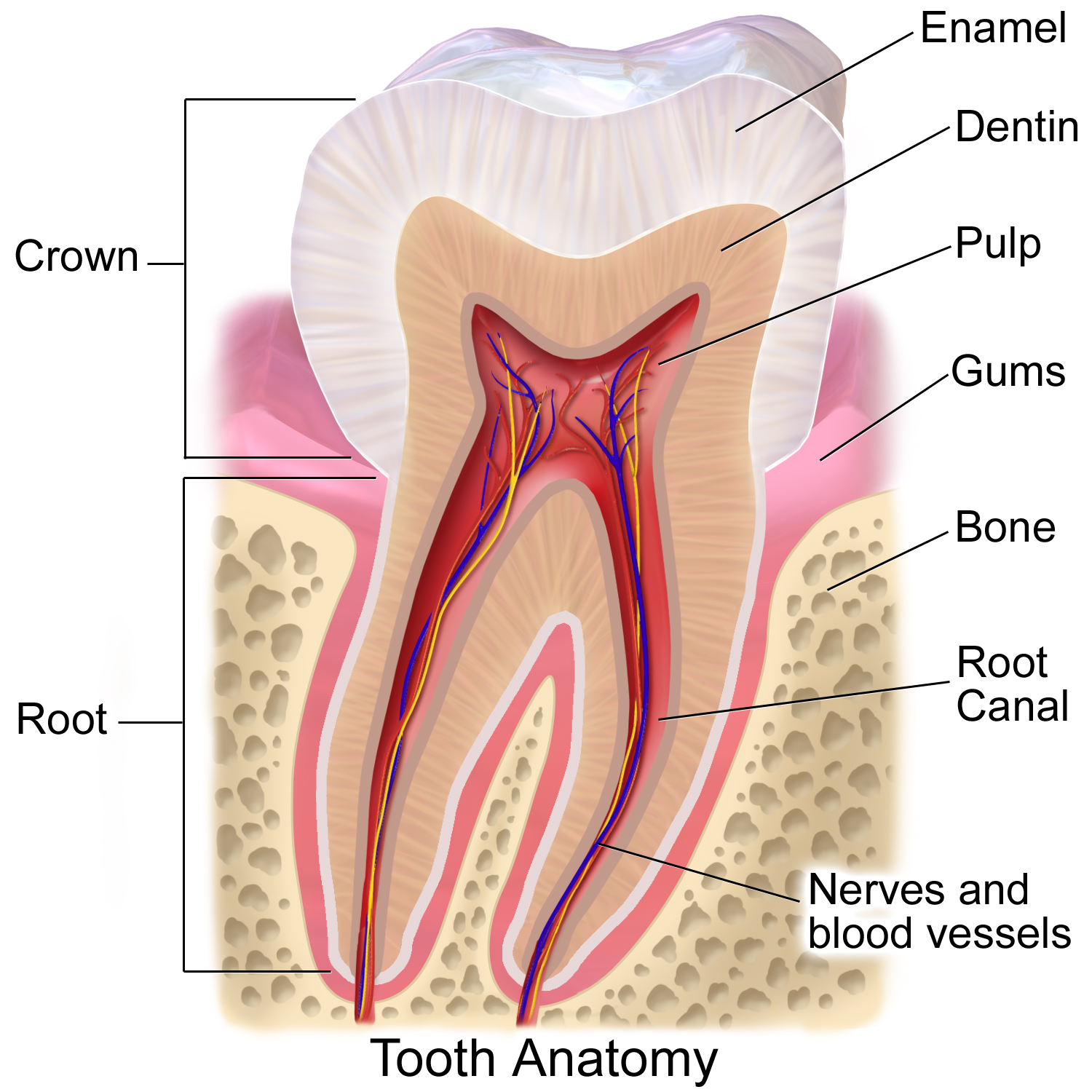
The gums or gingiva (pl.: gingivae) consist of the mucosal tissue that lies over the mandible and maxilla inside the mouth. Gum health and disease can have an effect on general health.
The gums are part of the soft tissue lining of the mouth. They surround the teeth and provide a seal around them. Unlike the soft tissue linings of the lips and cheeks, most of the gums are tightly bound to the underlying bone which helps resist the friction of food passing over them. Thus when healthy, it presents an effective barrier to the barrage of periodontal insults to deeper tissue. Healthy gums are usually coral pink in light skinned people, and may be naturally darker with melanin pigmentation.
Changes in color, particularly increased redness, together with swelling and an increased tendency to bleed, suggest an inflammation that is possibly due to the accumulation of bacterial plaque. Overall, the clinical appearance of the tissue reflects the underlying histology, both in health and disease. When gum tissue is not healthy, it can provide a gateway for periodontal disease to advance into the deeper tissue of the periodontium, leading to a poorer prognosis for long-term retention of the teeth. Both the type of periodontal therapy and homecare instructions given to patients by dental professionals and restorative care are based on the clinical conditions of the tissue.
The gums are divided anatomically into marginal, attached and interdental areas.
The marginal gum is the edge of the gums surrounding the teeth in collar-like fashion. In about half of individuals, it is demarcated from the adjacent, attached gums by a shallow linear depression, the free gingival groove. This slight depression on the outer surface of the gum does not correspond to the depth of the gingival sulcus but instead to the apical border of the junctional epithelium. This outer groove varies in depth according to the area of the oral cavity. The groove is very prominent on mandibular anteriors and premolars.
The marginal gum varies in width from 0.5 to 2.0 mm from the free gingival crest to the attached gingiva. The marginal gingiva follows the scalloped pattern established by the contour of the cementoenamel junction (CEJ) of the teeth. The marginal gingiva has a more translucent appearance than the attached gingiva, yet has a similar clinical appearance, including pinkness, dullness, and firmness. In contrast, the marginal gingiva lacks the presence of stippling, and the tissue is mobile or free from the underlying tooth surface, as can be demonstrated with a periodontal probe. The marginal gingiva is stabilized by the gingival fibers that have no bony support. The gingival margin, or free gingival crest, at the most superficial part of the marginal gingiva, is also easily seen clinically, and its location should be recorded on a patient's chart.
The attached gums are continuous with the marginal gum. It is firm, resilient, and tightly bound to the underlying periosteum of alveolar bone. The facial aspect of the attached gum extends to the relatively loose and movable alveolar mucosa, from which it is demarcated by the mucogingival junction. Attached gum may present with surface stippling. The tissue when dried is dull, firm, and immobile, with varying amounts of stippling. The width of the attached gum varies according to its location. The width of the attached gum on the facial aspect differs in different areas of the mouth. It is generally greatest in the incisor region (3.5 to 4.5 mm in the maxilla and 3.3 to 3.9 mm in the mandible) and less in the posterior segments, with the least width in the first premolar area (1.9 mm in the maxilla and 1.8 mm in the mandible). However, certain levels of attached gum may be necessary for the stability of the underlying root of the tooth.
The interdental gum lies between the teeth. They occupy the gingival embrasure, which is the interproximal space beneath the area of tooth contact. The interdental papilla can be pyramidal or have a "col" shape. Attached gums are resistant to the forces of chewing and covered in keratin.
Hub AI
Gums AI simulator
(@Gums_simulator)
Gums
The gums or gingiva (pl.: gingivae) consist of the mucosal tissue that lies over the mandible and maxilla inside the mouth. Gum health and disease can have an effect on general health.
The gums are part of the soft tissue lining of the mouth. They surround the teeth and provide a seal around them. Unlike the soft tissue linings of the lips and cheeks, most of the gums are tightly bound to the underlying bone which helps resist the friction of food passing over them. Thus when healthy, it presents an effective barrier to the barrage of periodontal insults to deeper tissue. Healthy gums are usually coral pink in light skinned people, and may be naturally darker with melanin pigmentation.
Changes in color, particularly increased redness, together with swelling and an increased tendency to bleed, suggest an inflammation that is possibly due to the accumulation of bacterial plaque. Overall, the clinical appearance of the tissue reflects the underlying histology, both in health and disease. When gum tissue is not healthy, it can provide a gateway for periodontal disease to advance into the deeper tissue of the periodontium, leading to a poorer prognosis for long-term retention of the teeth. Both the type of periodontal therapy and homecare instructions given to patients by dental professionals and restorative care are based on the clinical conditions of the tissue.
The gums are divided anatomically into marginal, attached and interdental areas.
The marginal gum is the edge of the gums surrounding the teeth in collar-like fashion. In about half of individuals, it is demarcated from the adjacent, attached gums by a shallow linear depression, the free gingival groove. This slight depression on the outer surface of the gum does not correspond to the depth of the gingival sulcus but instead to the apical border of the junctional epithelium. This outer groove varies in depth according to the area of the oral cavity. The groove is very prominent on mandibular anteriors and premolars.
The marginal gum varies in width from 0.5 to 2.0 mm from the free gingival crest to the attached gingiva. The marginal gingiva follows the scalloped pattern established by the contour of the cementoenamel junction (CEJ) of the teeth. The marginal gingiva has a more translucent appearance than the attached gingiva, yet has a similar clinical appearance, including pinkness, dullness, and firmness. In contrast, the marginal gingiva lacks the presence of stippling, and the tissue is mobile or free from the underlying tooth surface, as can be demonstrated with a periodontal probe. The marginal gingiva is stabilized by the gingival fibers that have no bony support. The gingival margin, or free gingival crest, at the most superficial part of the marginal gingiva, is also easily seen clinically, and its location should be recorded on a patient's chart.
The attached gums are continuous with the marginal gum. It is firm, resilient, and tightly bound to the underlying periosteum of alveolar bone. The facial aspect of the attached gum extends to the relatively loose and movable alveolar mucosa, from which it is demarcated by the mucogingival junction. Attached gum may present with surface stippling. The tissue when dried is dull, firm, and immobile, with varying amounts of stippling. The width of the attached gum varies according to its location. The width of the attached gum on the facial aspect differs in different areas of the mouth. It is generally greatest in the incisor region (3.5 to 4.5 mm in the maxilla and 3.3 to 3.9 mm in the mandible) and less in the posterior segments, with the least width in the first premolar area (1.9 mm in the maxilla and 1.8 mm in the mandible). However, certain levels of attached gum may be necessary for the stability of the underlying root of the tooth.
The interdental gum lies between the teeth. They occupy the gingival embrasure, which is the interproximal space beneath the area of tooth contact. The interdental papilla can be pyramidal or have a "col" shape. Attached gums are resistant to the forces of chewing and covered in keratin.
Recent media