
Community hub
Acinus
View on Wikipedia| Acinus | |
|---|---|
 Normal histology of the breast, including an acinus in lower image. The terminal duct connected to the magnified acinus is not within this microsection. | |
 Centroacinar cells | |
| Identifiers | |
| TH | H2.00.02.0.03050 |
| Anatomical terminology | |
An acinus (/ˈæsɪnəs/; pl.: acini; adjective, acinar /ˈæsɪnər/ or acinous) refers to any cluster of cells that resembles a many-lobed "berry", such as a raspberry (acinus is Latin for "berry"). The berry-shaped termination of an exocrine gland, where the secretion is produced, is acinar in form, as is the alveolar sac containing multiple alveoli in the lungs.
Exocrine glands
[edit]Acinar exocrine glands are found in many organs, including:
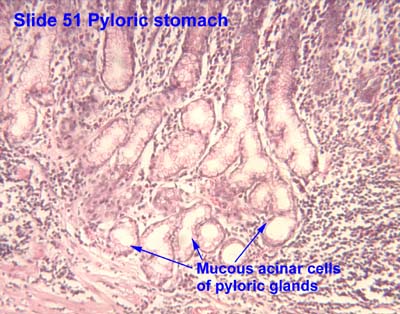
- the stomach[1]
- the sebaceous gland of the scalp
- the salivary glands of the tongue[2]
- the liver
- the lacrimal glands
- the mammary glands
- the pancreas[3]
- the bulbourethral (Cowper's) glands
The thyroid follicles can also be considered of acinar formation but in this case the follicles, being part of an endocrine gland, act as a hormonal deposit rather than to facilitate secretion.
Mucous acini usually stain pale, while serous acini usually stain dark.
Lungs
[edit]The end of the terminal bronchioles in the lungs mark the beginning of a pulmonary acinus that includes the respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli.[4]
See also
[edit]References
[edit]- ^ Histology image: 51_07 at the University of Oklahoma Health Sciences Center - pyloric stomach
- ^ Histology image: 46_03 at the University of Oklahoma Health Sciences Center - sublingual gland
- ^ Histology image:10405loa from Vaughan, Deborah (2002). A Learning System in Histology: CD-ROM and Guide. Oxford University Press. ISBN 978-0195151732.
- ^ Weinberger S (2019). Principles of Pulmonary Medicine. Elsevier. p. 2. ISBN 978-0-323-52371-4.
{kind=link}
{kind=link}
External links
[edit]
This anatomy article is a stub. You can help Wikipedia by expanding it. |