

Community hub
0 subscribers8 pages, 0 posts
Recent from talks
All channels
Be the first to start a discussion here.
Be the first to start a discussion here.
Be the first to start a discussion here.
Be the first to start a discussion here.
Contribute something
Welcome to the community hub built to collect knowledge and have discussions related to Coronal suture.
Nothing was collected or created yet.
Coronal suture
View on Wikipediafrom Wikipedia
| Coronal suture | |
|---|---|
 Anterolateral view of coronal suture (red) | |
| Details | |
| Part of | Skull |
| System | Skeletal |
| Nerve | Trigeminal nerve |
| Identifiers | |
| Latin | sutura coronalis |
| TA98 | A03.1.02.002 |
| TA2 | 1575 |
| FMA | 52928 |
| Anatomical terminology | |
The coronal suture is a dense, fibrous connective tissue joint that separates the two parietal bones from the frontal bone of the skull.
Structure
[edit]The coronal suture lies between the paired parietal bones and the frontal bone of the skull.[1] It runs from the pterion on each side.
Nerve supply
[edit]The coronal suture is likely supplied by a branch of the trigeminal nerve.[2]
Development
[edit]The coronal suture is derived from the paraxial mesoderm.
Clinical significance
[edit]If certain bones of the skull grow too fast then premature fusion of the sutures, craniosynostosis, may occur.[1] This can result in skull deformities.[1] These deformities include:[3]
- Brachycephaly (both sides)
- Plagiocephaly (one side only)
- Oxycephaly (both sides)
References
[edit]- ^ a b c Carlson, Bruce M. (2014-01-01). "9 - Integumentary, Skeletal, and Muscular Systems". Human Embryology and Developmental Biology (5th ed.). Saunders. pp. 156–192. doi:10.1016/b978-1-4557-2794-0.00009-7. ISBN 978-1-4557-2794-0.
- ^ Barral, Jean-Pierre; Croibier, Alain (2009-01-01). "2 - Characteristics of cranial nerves". Manual Therapy for the Cranial Nerves. Churchill Livingstone. pp. 7–14. ISBN 978-0-7020-3100-7.
- ^ "Craniosynostosis". Children's Hospitals and Clinics of Minnesota. 2015. Retrieved November 1, 2023.
- "Sagittal suture." Stedman's Medical Dictionary, 27th ed. (2000).
- Moore, Keith L., and T.V.N. Persaud. The Developing Human: Clinically Oriented Embryology, 7th ed. (2003).
Additional images
[edit]This gallery of anatomic features needs cleanup to abide by the medical manual of style. |
-
 Animation. Coronal suture shown in red.
Animation. Coronal suture shown in red. -

-
 Side view of the skull. ('Coronal suture' indicated by the arrow.)
Side view of the skull. ('Coronal suture' indicated by the arrow.) -
 Superior view of anterior part of the skull. Coronal suture runs horizontally.
Superior view of anterior part of the skull. Coronal suture runs horizontally. -
 Coronal suture seen from inside.
Coronal suture seen from inside. -
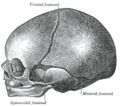 The skull at birth, showing the lateral fontanelle.
The skull at birth, showing the lateral fontanelle. -
 Coronal suture of new born baby.
Coronal suture of new born baby.







External links
[edit]Wikimedia Commons has media related to Coronal sutures.
- "Anatomy diagram: 34256.000-1". Roche Lexicon - illustrated navigator. Elsevier. Archived from the original on 2012-12-27.
- "Anatomy diagram: 34256.000-2". Roche Lexicon - illustrated navigator. Elsevier. Archived from the original on 2013-06-11.
Coronal suture
View on Grokipediafrom Grokipedia
The coronal suture is a dense and fibrous syndesmosis, or immovable joint, that connects the frontal bone to the two parietal bones across the superior aspect of the human skull.[1] It extends transversely from the pterion on each side, where it meets the sphenoparietal suture, to the midline bregma, where it intersects the sagittal suture, forming an oblique line that runs approximately from ear to ear.[1] In newborns, this suture allows for flexibility and slight movement of the skull plates during birth, while also permitting the cranium to expand symmetrically as the brain grows rapidly in infancy.[2] Derived embryologically from the paraxial mesoderm, the suture fuses around 24 years of age, after which it provides structural stability to the adult skull.[1]
Structurally, the coronal suture consists of interlocking bony edges bound by dense fibrous connective tissue, overlaid by the temporalis muscle and the epicranial aponeurosis, and it lies in close proximity to critical neurovascular structures such as the middle meningeal artery, which it helps protect.[1] Functionally, it plays a key role in accommodating brain volume increase during early development, contributing to the overall shaping of the calvaria.[1] Clinically, premature fusion of the coronal suture, known as coronal synostosis or craniosynostosis, is the second most common form of this condition and can lead to anterior plagiocephaly, characterized by a flattened forehead on the affected side, an elevated eye socket, and a deviated nose; bilateral involvement results in brachycephaly with a short, broad head shape.[3] Such early closure restricts cranial growth, potentially causing increased intracranial pressure, developmental delays, or neurological complications if untreated, often requiring surgical intervention in the first year of life to allow proper brain expansion.[3] Additionally, the region near the pterion along the coronal suture represents one of the skull's weakest points, making it vulnerable to trauma that could result in epidural hematoma.[1]