
Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Nasociliary nerve
View on Wikipedia| Nasociliary nerve | |
|---|---|
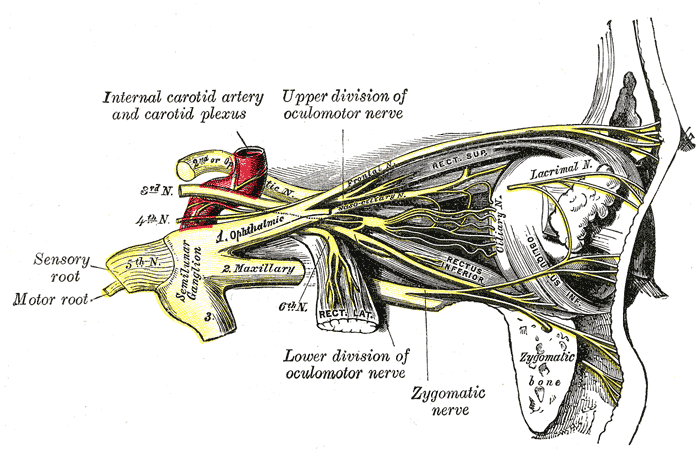
 Nerves of the orbit, and the ciliary ganglion. Side view. (Nasociliary is at center.) | |
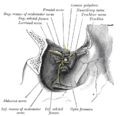
 Nerves of septum of nose. Right side. (Nasociliary is rightmost yellow line.) | |
| Details | |
| From | Ophthalmic nerve |
| To | Posterior ethmoidal nerve, anterior ethmoidal nerve, long ciliary nerves, infratrochlear nerve, communicating branch to ciliary ganglion |
| Identifiers | |
| Latin | nervus nasociliaris |
| TA98 | A14.2.01.025 |
| TA2 | 6204 |
| FMA | 52668 |
| Anatomical terms of neuroanatomy | |
The nasociliary nerve is a branch of the ophthalmic nerve (CN V1) (which is in turn a branch of the trigeminal nerve (CN V)). It is intermediate in size between the other two branches of the ophthalmic nerve, the frontal nerve and lacrimal nerve.[1]
Structure
[edit]Course
[edit]The nasociliary nerve enters the orbit via the superior orbital fissure,[citation needed] through the common tendinous ring,[1] and between the two heads of the lateral rectus muscle and between the superior and inferior rami of the oculomotor nerve.[citation needed] It passes across the optic nerve (CN II) along with the ophthalmic artery. It then runs obliquely beneath (inferior to) the superior rectus muscle and superior oblique muscle to the medial wall of the orbital cavity whereupon it emits the posterior ethmoidal nerve, and the anterior ethmoidal nerve.[1]
Branches
[edit]Branches of the nasociliary nerve include:[1]
Function
[edit]The branches of the nasociliary nerve provide sensory innervation to structures surrounding the eye such as the cornea, eyelids, conjunctiva, ethmoid air cells and mucosa of the nasal cavity.[citation needed]
Clinical significance
[edit]Clinical assessment
[edit]Since both the short and long ciliary nerves carry the afferent limb of the corneal reflex, one can test the integrity of the nasociliary nerve (and, ultimately, the trigeminal nerve) by examining this reflex in the patient. Normally both eyes should blink when either cornea (not the conjunctiva, which is supplied by the adjacent cutaneous nerves) is irritated. If neither eye blinks, then either the ipsilateral nasociliary nerve is damaged, or the facial nerve (CN VII, which carries the efferent limb of this reflex) is bilaterally damaged. If only the contralateral eye blinks, then the ipsilateral facial nerve is damaged. If only the ipsilateral eye blinks, then the contralateral facial nerve is damaged.[citation needed]
Additional images
[edit]-
 Nerves of the orbit. Seen from above.
Nerves of the orbit. Seen from above. -
 Distribution of the maxillary and mandibular nerves, and the submaxillary ganglion.
Distribution of the maxillary and mandibular nerves, and the submaxillary ganglion. -
 Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure.
Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure. -
 Pathways in the ciliary ganglion.
Pathways in the ciliary ganglion. -
 Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection.





References
[edit]- ^ a b c d Standring, Susan (2020). Gray's Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). New York. p. 782. ISBN 978-0-7020-7707-4. OCLC 1201341621.
{{cite book}}: CS1 maint: location missing publisher (link)
![]() This article incorporates text in the public domain from page 888 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 888 of the 20th edition of Gray's Anatomy (1918)
External links
[edit]- Anatomy figure: 29:03-08 at Human Anatomy Online, SUNY Downstate Medical Center - "A deeper dissection of the right orbit from a superior approach."
- lesson9 at The Anatomy Lesson by Wesley Norman (Georgetown University) (nasalseptumner)
- cranialnerves at The Anatomy Lesson by Wesley Norman (Georgetown University) (V)
- MedEd at Loyola GrossAnatomy/h_n/cn/cn1/cnb1.htm
{kind=link}
{kind=link}
Nasociliary nerve
View on GrokipediaAnatomy
Origin and course
The nasociliary nerve arises as one of the three principal branches of the ophthalmic division (V1) of the trigeminal nerve (cranial nerve V), originating from the medial aspect of the ophthalmic nerve near the trigeminal ganglion and within the lateral wall of the cavernous sinus.[5] It enters the orbit through the superior orbital fissure, passing within the annulus of Zinn (common tendinous ring), positioned between the superior and inferior divisions of the oculomotor nerve (CN III).[6][1] Within the orbit, the nasociliary nerve courses anteriorly in the intraconal space, traveling from lateral to medial superior to the optic nerve (approximately 8–12 mm anterior to the orbital apex) and between the superior oblique and medial rectus muscles.[5][2] It then pierces the myofascial cone to enter the extraconal space, extending along the medial orbital wall in close relation to the ophthalmic artery (with variable crossing patterns) and approaching the anterior ethmoidal foramen.[1][6] The nerve maintains proximity to the trochlea via its anterior course and to the ethmoidal foramina, through which related pathways extend into the cranial cavity.[2][5] Anatomical variations of the nasociliary nerve include occasional communications with adjacent nerves, such as the lacrimal nerve, and potential extensions of its branches to nearby extraocular muscles like the superior rectus or medial rectus.[7] Additionally, the posterior ethmoidal component may be absent in about 30% of individuals, altering the nerve's distribution along the medial wall.[6]Branches and relations
The nasociliary nerve issues multiple branches as it courses through the orbit, primarily distributing along its medial and anterior paths. These include the long ciliary nerves, typically numbering two or three, which arise near the posterior orbit and pierce the sclera medial to the optic nerve to reach the interior structures of the eyeball.[3][2] Further anteriorly, the posterior ethmoidal nerve emerges from the nasociliary nerve and passes through the posterior ethmoidal foramen to connect with the posterior ethmoidal air cells, sphenoidal sinus, and adjacent dura mater.[3][7] The anterior ethmoidal nerve branches off near the anterior orbit, traversing the anterior ethmoidal foramen to reach the anterior ethmoidal air cells and nasal cavity mucosa; it continues as the external nasal branch, emerging onto the external surface to connect with the skin of the nasal bridge.[3][2][7] The infratrochlear nerve arises from the anterior portion of the nasociliary nerve, directing inferiorly and anteriorly below the trochlea to reach the medial orbital structures, including the skin of the medial upper eyelid, lacrimal sac, and caruncle.[3][2] Additionally, the long root of the ciliary ganglion branches from the nasociliary nerve posteriorly, joining the ciliary ganglion located near the orbital apex.[2][8] In terms of communications, the nasociliary nerve connects with the ciliary ganglion via its long root, allowing passage of fibers through the ganglion without relay.[2][8] It also establishes connections with the pterygopalatine ganglion indirectly through branches of the anterior ethmoidal nerve.[3] Anastomoses with the lacrimal nerve have been observed in some cases.[7] Anatomically, the nasociliary nerve maintains relations with key orbital elements: it travels superior to the optic nerve and between the superior oblique and medial rectus muscles intraconaly, then pierces the myofascial cone to run along the medial orbital wall extraconaly.[1][2] Superiorly, it relates to the frontal nerve, while inferiorly it is positioned relative to the lacrimal nerve within the broader ophthalmic division distribution.[3][1]Function
Sensory innervation
The nasociliary nerve, a branch of the ophthalmic division of the trigeminal nerve (CN V1), provides somatic sensory innervation to several structures in the nasal and ocular regions, including the nasal mucosa, ethmoidal and sphenoidal sinuses, medial conjunctiva, skin of the root and tip of the nose, and lacrimal sac.[6][9] These sensory fibers convey general sensations such as touch, pain, and temperature from these areas, contributing to the protective and perceptual functions of the trigeminal system without any motor components.[10] Specific branches of the nasociliary nerve mediate targeted sensory supply. The anterior ethmoidal nerve innervates the mucosa of the anterior nasal septum and the superior turbinate, as well as the anterior and middle ethmoidal air cells.[6] The infratrochlear nerve supplies sensation to the medial canthus, including the skin of the medial eyelids, medial conjunctiva, lacrimal sac, and caruncle.[6] The long ciliary nerves provide sensory innervation to the corneal stroma, iris, and ciliary body, transmitting afferent signals for corneal protection and ocular surface integrity.[8] Additionally, the posterior ethmoidal nerve contributes to sensory input from the posterior ethmoidal cells and sphenoidal sinus mucosa.[9] The nasociliary nerve participates in referred pain pathways within the trigeminal distribution, where irritation in its sensory territories—such as the nasal mucosa or sinuses—can project pain to the forehead, medial orbit, or nasal skin due to convergence of trigeminal afferents in the trigeminal ganglion and brainstem nuclei.[10] This mechanism underlies symptoms in conditions involving trigeminal activation, occurring exclusively through sensory fibers without motor involvement.[11] Through its sensory afferents, the nasociliary nerve contributes to autonomic reflex arcs, providing the afferent limb for reflexes such as the nasolacrimal reflex, where nasal mucosal stimulation triggers lacrimation via connections to parasympathetic pathways in the brainstem.[12] This reflex integrates sensory input from nasal and ocular regions to facilitate protective tearing responses.[12]Autonomic interactions
The nasociliary nerve serves as a conduit for postganglionic sympathetic fibers originating from the superior cervical ganglion, which travel via the internal carotid plexus and join the nerve within the orbit. These fibers distribute primarily through the long ciliary nerves to innervate the dilator pupillae muscle, facilitating pupillary dilation, and extend to the nasal mucosa via branches such as the anterior ethmoidal nerve for vasomotor control, including vasoconstriction to regulate nasal patency. Unlike parasympathetic fibers, these sympathetic fibers do not synapse within peripheral ganglia along their path but pass through the ciliary ganglion uninterrupted when associated with short ciliary nerves, acting as a pure relay station.[8] Parasympathetic contributions to the nasociliary nerve occur indirectly through communications with the pterygopalatine ganglion, where preganglionic fibers from the facial nerve (CN VII) synapse to produce postganglionic fibers that join nasociliary branches, particularly the ethmoidal nerves.[13] These fibers promote nasal vasodilation and glandular secretion in the nasal mucosa, contributing to mucus production and mucosal hydration. A 2025 cadaveric study identified sensory, parasympathetic, and sympathetic nerve markers in the anterior ethmoidal nerve, supporting its role in vasomotor control.[13] Although the nasociliary nerve itself does not directly carry parasympathetic input to the lacrimal gland—that role belongs to the lacrimal nerve via zygomatic communications—its proximity and shared orbital pathways allow for integrated autonomic effects on lacrimal secretion in response to nasal stimuli. Sensory fibers from the nasociliary nerve pass through the ciliary ganglion without synapsing, preserving their role in general sensation while facilitating autonomic relay. Functionally, the integration of sensory and autonomic components in the nasociliary nerve enables reflex arcs where sensory input from nasal or ocular mucosa triggers autonomic responses. For instance, irritation detected by nasociliary sensory afferents can activate parasympathetic outflow via central connections, leading to nasal congestion reflexes involving increased vasodilation and secretion. Sympathetic modulation counterbalances this by promoting vasoconstriction, maintaining nasal airflow homeostasis. This sensory-autonomic interplay underscores the nerve's role in protective reflexes without direct synaptic interruption in peripheral ganglia.[3]Clinical significance
Pathological involvement
The nasociliary nerve is implicated in cluster headaches through activation of the trigeminal-autonomic reflex, where its sensory afferents from the ophthalmic division (V₁) of the trigeminal nerve contribute to the orbital and supraorbital pain, while triggering ipsilateral autonomic symptoms such as lacrimation and nasal congestion via parasympathetic outflow.[15][16] This reflex pathway involves hypothalamic activation leading to secondary trigeminal nerve stimulation, with the nasociliary branch playing a key role in mediating the ocular and nasal sensory inputs that exacerbate the episodic, severe unilateral attacks characteristic of the condition.[17] In herpes zoster ophthalmicus, reactivation of the varicella-zoster virus along the ophthalmic division of the trigeminal nerve frequently involves the nasociliary branch, resulting in intense pain in its distribution and a heightened risk of ocular complications.[18] The presence of vesicles on the nasal tip, known as Hutchinson's sign, specifically indicates nasociliary involvement and correlates with a threefold increased likelihood of intraocular inflammation.[19] This can lead to corneal denervation and ulceration through the long ciliary nerves, which supply sensory innervation to the cornea, potentially progressing to neurotrophic keratitis if untreated.[20][21] Inflammation of the ethmoidal sinuses in sinusitis or rhinosinusitis often affects the anterior and posterior ethmoidal branches of the nasociliary nerve, causing referred pain to the nasal cavity, medial orbit, and forehead due to irritation of these sensory fibers.[9] Such involvement underscores the nerve's role in transmitting nociceptive signals from sinus pathology, distinguishing it from broader maxillary or frontal sinus referrals.[22] Rare pathological conditions such as tumors, infections, or trauma at the superior orbital fissure can compress or inflame the nasociliary nerve, contributing to orbital apex syndrome characterized by ophthalmoplegia, ptosis, and sensory loss in the V₁ distribution.[23] In this syndrome, the nerve's passage through the middle portion of the fissure alongside oculomotor and abducens nerves leads to combined cranial neuropathies, with nasociliary involvement manifesting as corneal anesthesia and reduced blink reflex.[24] Historical observations, such as Jonathan Hutchinson's 1865 description in herpes zoster ophthalmicus, highlighted the nerve's shared innervation of the nasal tip, cornea, and iris, providing a basis for understanding zoster-related and idiopathic nasal pains as neuralgic phenomena originating from this branch. These observations in period texts, along with early 20th-century descriptions of nasociliary neuralgia, emphasized the nerve's vulnerability to inflammatory and traumatic insults, predating modern classifications of trigeminal branch-specific neuralgias.[5][25]Diagnostic and therapeutic considerations
Clinical assessment of nasociliary nerve function typically involves sensory testing of the nasal mucosa using a cotton swab to evaluate touch and pain responses in the distribution of its internal nasal and anterior ethmoidal branches.[26] The corneal reflex, mediated by the long ciliary branches of the nasociliary nerve, is tested by gently touching the cornea with a twisted cotton wisp, eliciting a bilateral blink response if intact.[27] For suspected orbital involvement, computed tomography (CT) and magnetic resonance imaging (MRI) are employed to visualize nerve compression, perineural spread, or structural abnormalities, with MRI preferred for soft tissue detail and CT for bony structures.[28][29] Diagnostic tools include trigeminal somatosensory evoked potentials to assess nerve conduction along the nasociliary pathway, particularly in cases of suspected neuropathy.[30] Nasal endoscopy facilitates direct visualization of mucosal irritation or inflammation potentially affecting the nerve's sensory distribution.[31] Therapeutic interventions for nasociliary nerve-related disorders encompass local anesthetic nerve blocks targeting the external nasal or anterior ethmoidal branches to alleviate pain in conditions such as cluster headache or Charlin's syndrome.[32] Antiviral agents like acyclovir are administered for herpes zoster ophthalmicus involving the nasociliary nerve to reduce viral replication and prevent complications.[10] In trauma-induced compression, surgical decompression via orbital approaches may be performed to relieve pressure on the nerve.[33] As of 2025, emerging neuromodulation techniques, including peripheral nerve stimulation of trigeminal branches, offer targeted relief for chronic nasal pain refractory to conventional therapies.[34] These devices modulate pain signals electrically, showing promise in clinical trials for trigeminal neuropathies.[35] Diagnostic and therapeutic challenges arise from the nasociliary nerve's overlap with other ophthalmic division (V₁) branches, necessitating differential diagnosis through combined clinical and imaging evaluations to isolate involvement.[36]References
- https://www.sciencedirect.com/topics/[neuroscience](/page/Neuroscience)/nasociliary-nerve