

Community hub
Recent from talks
Contribute something
Nothing was collected or created yet.
Nasalis muscle
View on Wikipedia| Nasalis muscle | |
|---|---|
 The superior transverse part and inferior alar part of the nasalis muscle | |
| Details | |
| Origin | Maxilla |
| Insertion | Nasal bone |
| Artery | Superior labial artery |
| Nerve | Buccal branch of the facial nerve |
| Actions | Compresses bridge of nose, depresses tip of nose, elevates corners of nostrils |
| Identifiers | |
| Latin | musculus nasalis |
| TA98 | A04.1.03.009 |
| TA2 | 2062 |
| FMA | 46770 |
| Anatomical terms of muscle | |
The nasalis muscle is a sphincter-like muscle of the nose. It has a transverse part and an alar part. It compresses the nasal cartilages, and can "flare" the nostrils. It can be used to test the facial nerve (VII), which supplies it.
Structure
[edit]The nasalis muscle covers the nasal cartilages of the lower surface of the nose.[1] It consists of two parts, transverse and alar:
- The transverse part (compressor naris muscle) arises from the maxilla, above and lateral to the incisive fossa. Its fibers proceed upward and medially, expanding into a thin aponeurosis which is continuous on the bridge of the nose with that of the muscle of the opposite side, and with the aponeurosis of the procerus muscle. It compresses the nostrils and may completely close them.[2]
- The alar part (dilator naris muscle) arises from the maxilla over the lateral incisor and inserts into the greater alar cartilage. Its medial fibres tend to blend with the depressor septi nasi muscle, and has been described as part of that muscle.
Nerve supply
[edit]Like all the other muscles of facial expression, the nasalis muscle is supplied by the facial nerve (VII).[3][4]
Function
[edit]The nasalis muscle compresses the nasal cartilages. It may also "flare" the nostrils.[2]
Clinical significance
[edit]Cleft lip and cleft palate
[edit]The nasalis muscle is one of the key muscles not formed or inserted correctly with cleft lip and cleft palate deformity.[5] The head of the transverse part needs to be identified during reconstructive surgery so that it can be surgically sutured (connected) to the nasal septum.[2][5] The origin at the maxilla may also be repositioned for better symmetry.[2]
Facial nerve testing
[edit]Due to it being superficial, the nasalis muscle can be used to test the facial nerve.[4][6] Specifically, it can be used to test the zygomatic branches.[6]
Additional images
[edit]-
 Muscles of the head, face, and neck. (Nasalis labeled at center left.)
Muscles of the head, face, and neck. (Nasalis labeled at center left.) -
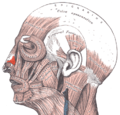
 Position of nasalis muscle (shown in red).
Position of nasalis muscle (shown in red).


References
[edit]- ^ Menick, Frederick J. (2009). "Small Superficial Defects — Secondary Intention Healing, Primary Repair, a Skin Graft or Local Flap". Nasal Reconstruction. pp. 65–90. doi:10.1016/B978-0-7020-3008-6.50010-7. ISBN 978-0-7020-3008-6. OCLC 460904328.
- ^ a b c d Attia, Sarah A.; Helal, Hesham A.; El Barabary, Amir S.; Awad, Mostafa A.; Sherif, Mahmoud M. (February 2019). "Impact of nasalis muscle repair in unilateral cleft lip patients". Journal of Cranio-Maxillofacial Surgery. 47 (2): 255–262. doi:10.1016/j.jcms.2018.11.030. PMID 30591393.
- ^ "Nasalis". www.anatomynext.com. Archived from the original on 2018-03-01. Retrieved 2018-03-01.
- ^ a b Sanders, Donald B. (2012). "Electrophysiologic Study of Disorders of Neuromuscular Transmission". Aminoff's Electrodiagnosis in Clinical Neurology. pp. 385–406. doi:10.1016/B978-1-4557-0308-1.00017-0. ISBN 978-1-4557-0308-1. OCLC 793587054.
- ^ a b Drake, David; Colbert, Serryth (2017). "Techniques for Cleft Lip Repair". Maxillofacial Surgery. pp. 948–971. doi:10.1016/B978-0-7020-6056-4.00067-8. ISBN 978-0-7020-6056-4. OCLC 968339962.
- ^ a b Preston, David C.; Shapiro, Barbara E. (2013). "Facial and Trigeminal Neuropathy". Electromyography and Neuromuscular Disorders. pp. 372–383. doi:10.1016/B978-1-4557-2672-1.00025-8. ISBN 978-1-4557-2672-1. OCLC 821857515.
External links
[edit]Nasalis muscle
View on GrokipediaAnatomy
Origin and insertion
The nasalis muscle consists of two parts: the transverse part (compressor naris) and the alar part (dilator naris), which together form a paired structure spanning the nasal region.[1] The transverse part originates from the maxilla superolateral to the incisive fossa. Its fibers course superiorly and medially, inserting into a transverse aponeurosis across the bridge of the nose, where they interconnect with the fibers of the contralateral transverse part.[2][4] The alar part originates from the maxilla superior to the root of the lateral incisor tooth. The muscle fibers then pass inferiorly and laterally to insert primarily into the greater alar cartilage and the adjacent skin of the nostril margin, with some fibers extending to blend with the transverse part.[1][2] Overall, the nasalis muscle is thin and strap-like, forming a functional sling around the nasal aperture.[5] In standard anatomical nomenclature, the nasalis muscle is designated as TA98: A04.1.03.009, TA2: 2062, and FMA: 46770.[6]Relations
The nasalis muscle is situated deep to the nasal skin and superficial to the underlying nasal cartilages and bones, integrating into the superficial musculoaponeurotic system (SMAS) of the nasal region.[1][7] As part of the nasal musculature, it contributes to the sphincter-like mechanism around the nasal aperture, interconnecting with adjacent soft tissues via the nasal SMAS aponeurosis.[8] The transverse part of the nasalis muscle covers the dorsum of the nose, lying superficial to the lateral nasal cartilage and blending medially with its contralateral counterpart at the midline.[1] Superiorly, it merges with the aponeurosis of the procerus muscle at the nasal bridge.[7] Laterally, its fibers interdigitate with those of the levator labii superioris alaeque nasi muscle along the sides of the nose.[7] The alar part originates over the maxilla and attaches to the greater alar cartilage, particularly the lateral crus, occupying much of the alar region and supporting the soft tissue hinge area of the nasal valve.[9] It lies lateral to the depressor septi nasi muscle and may interconnect with it inferiorly through shared fibrous expansions in some variations.[1] Laterally, it also blends with fibers of the levator labii superioris alaeque nasi, facilitating coordinated movement within the nasal musculature.Innervation
The nasalis muscle is innervated by the buccal branch of the facial nerve (cranial nerve VII), which arises from the parotid plexus within the parotid gland.[11][1] This branch provides motor innervation to both the transverse and alar parts of the muscle, enabling coordinated actions such as nostril compression and dilation.[2] The facial nerve originates in the pons at the pontomedullary junction, where motor fibers emerge from the facial motor nucleus and exit the brainstem alongside the nervus intermedius.[11] It travels through the facial canal in the temporal bone before emerging from the skull via the stylomastoid foramen, then courses anteriorly through the parotid gland, dividing into temporofacial and cervicofacial trunks at the pes anserinus. The buccal branch specifically emerges from the cervicofacial division and travels forward across the buccinator muscle to reach the nasalis.[11] Nerve fibers from this branch enter the nasalis muscle on its deep surface, consistent with the general pattern for muscles of facial expression.[11][12] As a lower facial muscle, the nasalis receives unilateral (ipsilateral) innervation from upper motor neurons via the corticobulbar tract, which permits independent control and movement of each nostril, such as unilateral flaring during facial expressions or respiration.[11] This motor function can be assessed in clinical evaluations of facial nerve integrity.[3]Blood supply
The nasalis muscle receives its arterial supply from the superior labial, septal, and lateral nasal branches of the facial artery, as well as the infraorbital branch of the maxillary artery.[1][2] The superior labial artery, a branch of the facial artery that arises near the angle of the mouth and ascends along the upper lip, supplies the nasal base and surrounding structures.[1] This vessel provides oxygenated blood to the muscle's attachments at the nasal base, ensuring adequate perfusion for its contractile functions.[13] The transverse part of the nasalis muscle, also known as the compressor naris, receives contributions from the lateral nasal artery, another branch of the facial artery that emerges superior to the superior labial artery and courses along the lateral aspect of the nose to vascularize the external nasal sidewall.[14] This targeted supply supports the transverse portion's role in compressing the nasal apertures.[2] Venous drainage of the nasalis muscle parallels its arterial supply, with corresponding superior labial and lateral nasal veins collecting deoxygenated blood and emptying into the facial vein, which ultimately drains into the internal jugular vein via the common facial vein.[15] These venous tributaries follow a superficial course, facilitating efficient return of blood from the nasal region.[16] Due to the nasalis muscle's superficial position overlying the nasal cartilages, it benefits from collateral arterial supply via anastomoses with branches of the angular artery, the terminal extension of the facial artery that ascends along the medial nasal side to interconnect with the dorsal nasal artery from the ophthalmic artery.[8] This network enhances vascular redundancy in the perinasal area.[14]Function
Transverse part
The transverse part of the nasalis muscle, also known as the compressor naris, originates from the maxilla above and lateral to the incisive fossa and inserts via a thin aponeurosis that bridges the dorsum of the nose, merging with its contralateral counterpart.[17][1] Its primary action is to compress the nasal aperture by drawing the greater alar cartilages medially toward the nasal septum, thereby narrowing the nostrils and reducing the nasal opening.[17][18] This compressive function helps regulate airflow through the nose and prevents collapse of the nasal valve during certain respiratory efforts.[19] In addition to narrowing the nostrils, contraction of the transverse part contributes to wrinkling the skin over the nasal dorsum and bridge, producing visible transverse furrows that are characteristic of certain facial expressions.[17][1] When both transverse parts contract bilaterally, they act in concert to form a functional sphincter around the nasal aperture, encircling and constricting the external nares in a ring-like manner.[17][20] This sphincteric action enhances the muscle's role in modulating nasal patency.[7] Electromyographic studies have demonstrated activation of the transverse part during forced inspiration, particularly in individuals with reduced nasal patency, where it works to maintain airway openness alongside other nasal muscles.[19] Furthermore, surface electromyography recordings show increased activity in the nasalis muscle, including its transverse portion, in response to unpleasant odors that elicit emotional expressions such as disgust, contributing to the associated nasal wrinkling and compression.[21][7] These findings underscore the transverse part's involvement in both respiratory biomechanics and expressive functions.[19]Alar part
The alar part of the nasalis muscle, also known as the dilator naris posterior, primarily functions to dilate the nostrils by pulling the alar cartilages laterally and inferiorly, thereby increasing nasal airflow during inhalation.[1] This action depresses the ala nasi laterally while widening the nasal aperture, facilitating greater air intake without compressing the nasal structures.[1] It inserts into the greater alar cartilage and the overlying skin, enabling this expansive movement.[22] In addition to dilation, the alar part expands the lateral nasal wall by stiffening the alar region, contributing to nostril flaring observed during deep breathing or physical exertion when oxygen demand increases.[23] This expansion assists in maintaining an open nasal passage under heightened respiratory effort, such as during exercise, by stiffening and expanding the alar region. The muscle's contraction in these scenarios enhances overall nasal patency, supporting efficient ventilation.[2] The alar part can contract independently on each side, allowing for asymmetric nostril widening, which is evident in unilateral activation during facial movements or diagnostic assessments.[1] This bilateral yet separable function permits targeted dilation without symmetric involvement, aiding in nuanced control of airflow.[23] It integrates with accessory dilators, such as the dilator naris anterior and dilator naris vestibularis, to achieve enhanced nostril aperture expansion during coordinated nasal dilation.[23] These synergistic actions amplify the alar part's role in dynamic nasal opening, particularly in response to varying respiratory needs.Development and variations
Embryology
The nasalis muscle originates from the mesoderm of the second pharyngeal arch, which forms during the fourth week of embryonic development. Myoblasts from this arch migrate ventrally along the course of the facial nerve (cranial nerve VII) precursors to innervate the developing facial structures, including the nasal region.[24][25] This migration establishes the foundational innervation and positioning of the nasalis as part of the broader group of facial expression muscles.[26] Between embryonic weeks 6 and 10, the nasalis muscle forms in conjunction with the fusion of the frontonasal prominence, where myoblasts invade the nasal mesenchyme to differentiate into muscle fibers. The nasal placodes, appearing around week 5, invaginate to form nasal pits, contributing to the spatial organization of the nasal structures and guiding the positioning of the emerging nasalis precursors. By week 10, the transverse and alar components of the nasalis differentiate within this mesenchyme, aligning with the overall shaping of the midface.[24][27][28][8] Postnatally, newborns are obligatory nose breathers, placing demands on nasal structures for airflow, though specific maturation details of the nasalis muscle remain limited in the literature.[29]Anatomical variations
The nasalis muscle exhibits several anatomical variations, primarily involving accessory muscular slips and alterations in its topographic relationships. Thin muscular slips along the outer margins of the nostrils are occasionally observed as distinct structures, termed dilatores naris anterior and posterior, which extend from the alar part toward the upper lip and contribute to nostril dilation.[30] These slips, described in classical anatomical texts, represent minor accessory bands that may vary in presence and extent among individuals.[30] A rare variant known as the anomalous nasi muscle has been documented in cadaveric dissections, originating from the frontal process of the maxilla medial to the levator labii superioris alaeque nasi and blending with the deep and lateral fibers of the procerus muscle. This inconstant structure measures approximately 11.9 mm in length and 2.8 mm in width, lying on the lateral side of the nose without a direct connection to the standard nasalis components.[31] Topographic variations in the nasalis muscle often involve the alar part and associated dilator components, such as the dilator naris vestibularis and dilator naris anterior, which may show altered insertions or fiber arrangements affecting nasal valve function. For instance, the dilator naris anterior can originate variably from the lateral crus or accessory alar cartilage and insert into the alar groove, while the dilator naris vestibularis radiates fibers along the nasal vestibule with potential deviations in its dome-shaped distribution. These variations, observed in embalmed cadavers, highlight differences in muscular topography that influence nasal dynamics.[32] Asymmetry in the nasalis muscle, including unilateral hypoplasia, occurs in some cases and is associated with broader facial asymmetries, though specific prevalence data for this muscle remain limited in the literature.[30]Clinical significance
Cleft lip and palate
In unilateral cleft lip, the continuity of the nasalis muscle is disrupted due to the failure of fusion between the medial and lateral nasal prominences during embryonic development, resulting in abnormal insertions that displace the alar base laterally and cause a flattened nostril shape with excessive alar flaring.[33] This muscle imbalance pulls the lower lateral cartilage outward, widening the nasal floor and contributing to overall nasal asymmetry. In bilateral clefts, the nasalis muscle exhibits symmetric discontinuity of the nasolabial muscular ring, with bilateral aberrant insertions leading to splayed alae, a broad and flat nasal tip, and a short, retruded columella that exacerbates the nasal deformity.[34] The lack of muscular continuity across the prolabium prevents normal support of the nasal structures, resulting in lateral displacement of the alar bases and a bifid nasal appearance.[33] Primary surgical repair of these deformities, typically performed between 3 and 6 months of age, focuses on restoring the nasalis muscular ring through techniques such as the Millard rotation-advancement method, which involves wide dissection to release the nasalis from its abnormal insertions, followed by repositioning and suturing of the muscle fibers to the contralateral side or midline structures like the septum to reestablish continuity.[33] An alar cinch suture is often employed to medialize the alar bases, narrowing the nasal floor and supporting the repositioned nasalis for improved structural alignment.[35] Long-term outcomes following nasalis reconstruction demonstrate enhanced nasal symmetry, with reduced alar base width and improved columellar height and nasal tip projection approaching non-cleft norms, as evidenced by randomized trials showing statistically significant corrections in nostril angles and overall nasal form.[36] These repairs also mitigate progressive deformities, promoting better functional nasal airflow and aesthetic balance into adolescence.[33]Facial nerve testing
The nasalis muscle is clinically assessed during facial nerve (cranial nerve VII) examination by observing nostril flaring, either on verbal command or during deep inspiration, to evaluate contractility; unilateral weakness or asymmetry in this movement suggests a lesion in the buccal branch of the facial nerve.[37][38] In the evaluation of Bell's palsy, asymmetric contraction of the nasalis muscle, observed as reduced or absent nostril flaring on the affected side, indicates involvement of the lower division of the facial nerve, helping differentiate peripheral from central lesions.[39] Electromyography (EMG) of the nasalis muscle is a key diagnostic tool for confirming denervation in facial paralysis, with needle EMG detecting pathologic spontaneous activity such as fibrillation potentials and positive sharp waves approximately 10–14 days after injury, signaling axonal degeneration.[40] Recovery patterns are monitored via EMG, where signs of reinnervation, including polyphasic motor unit action potentials, typically emerge 3–6 months post-injury, often preceding visible clinical improvement by several months.[40] Electroneurography (ENoG) targeting the nasalis, performed 2–4 weeks after symptom onset, provides prognostic insight, with amplitudes below 92.5% of normal associated with poorer outcomes at 2 months in severe cases.[41][42] Due to its superficial position along the nasal ala, the nasalis muscle permits non-invasive palpation during neurological exams; the examiner places a finger lateral to the nose and requests nostril flaring to assess contractility and symmetry directly.[37]Surgical considerations
In rhinoplasty procedures aimed at addressing aesthetic concerns, hypertrophic transverse portions of the nasalis muscle may be partially resected to mitigate the appearance of bunny-line wrinkles, which result from repetitive contraction of this muscle along the nasal dorsum.[43] The open rhinoplasty approach facilitates direct exposure of the muscle through a transcolumellar incision, allowing for precise partial myectomy while preserving surrounding structures to maintain nasal function.[43] During septoplasty, preservation of the nasalis muscle is essential to avoid postoperative nasal obstruction due to alar collapse, as electromyographic (EMG) studies demonstrate reduced muscle activity following dissection, which impairs the dilatory function critical for maintaining airway patency.[44] This temporary decrease in nasalis activation, observed in postoperative evaluations, underscores the need for subperichondrial dissection techniques to minimize iatrogenic disruption.[44] In nasal valve surgery, the alar part of the nasalis muscle can be reinforced using suture suspension or cartilage grafts to counteract dynamic collapse during inspiration, thereby widening the external nasal valve and improving airflow.[45] Techniques such as alar batten grafts or expansion sutures anchor to the lateral crura, enhancing the supportive role of the alar nasalis in stabilizing the nasal sidewall, with reported airway improvements in over 90% of cases.[45] Surgical interventions involving the nasalis carry risks of iatrogenic denervation from facial nerve branch injury, potentially leading to facial asymmetry through weakened nasal flaring and tip depression.[46] However, the muscle's robust collateral circulation from branches of the facial and angular arteries typically minimizes the risk of ischemia, supporting rapid recovery of function in most instances.[47]References
- https://www.wikidata.org/wiki/Q597112
- https://www.sciencedirect.com/topics/[neuroscience](/page/Neuroscience)/nasalis-muscle