
Community hub
0 subscribers8 pages, 0 posts
Recent from talks
All channels
Be the first to start a discussion here.
Be the first to start a discussion here.
Be the first to start a discussion here.
Be the first to start a discussion here.
Contribute something
Welcome to the community hub built to collect knowledge and have discussions related to Ventricular flutter.
Nothing was collected or created yet.
Ventricular flutter
View on Wikipediafrom Wikipedia
| Ventricular flutter | |
|---|---|
 | |
| Specialty | Cardiology |
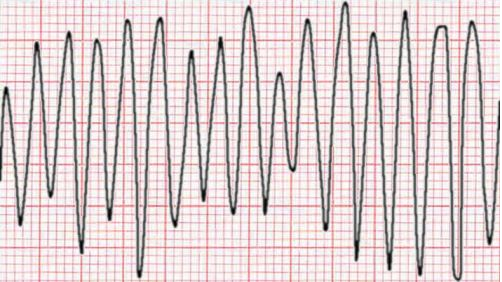
Ventricular flutter is an arrhythmia, more specifically a tachycardia affecting the ventricles with a rate over 250-350 beats/min, and one of the most indiscernible. It is characterized on the ECG by a sinusoidal waveform without clear definition of the QRS and T waves. It has been considered as a possible transition stage between ventricular tachycardia and fibrillation, and is a critically unstable arrhythmia that can result in sudden cardiac death.[citation needed][1]
It can occur in infancy,[2] youth,[3] or as an adult.
It can be induced by programmed electrical stimulation.[4][5]
References
[edit]- ^ "Heart Ventricle Flutter - an overview | ScienceDirect Topics". www.sciencedirect.com. Retrieved 2023-05-11.
- ^ Thies KC, Boos K, Müller-Deile K, Ohrdorf W, Beushausen T, Townsend P (January 2000). "Ventricular flutter in a neonate--severe electrolyte imbalance caused by urinary tract infection in the presence of urinary tract malformation". J Emerg Med. 18 (1): 47–50. doi:10.1016/S0736-4679(99)00161-4. PMID 10645837.
- ^ Hayashi M, Murata M, Satoh M, et al. (July 1985). "Sudden nocturnal death in young males from ventricular flutter". Jpn Heart J. 26 (4): 585–91. doi:10.1536/ihj.26.585. PMID 4057556.
- ^ Gurevitz O, Viskin S, Glikson M, et al. (April 2004). "Long-term prognosis of inducible ventricular flutter: not an innocent finding". Am. Heart J. 147 (4): 649–54. doi:10.1016/j.ahj.2003.11.012. PMID 15077080.
- ^ Viskin S, Ish-Shalom M, Koifman E, et al. (September 2003). "Ventricular flutter induced during electrophysiologic studies in patients with old myocardial infarction: clinical and electrophysiologic predictors, and prognostic significance". J. Cardiovasc. Electrophysiol. 14 (9): 913–9. doi:10.1046/j.1540-8167.2003.03082.x. PMID 12950532. S2CID 30924977.
External links
[edit]
This medical symptom article is a stub. You can help Wikipedia by expanding it. |
Ventricular flutter
View on Grokipediafrom Grokipedia