Recent from talks
Bearded lady
Knowledge base stats:
Talk channels stats:
Members stats:
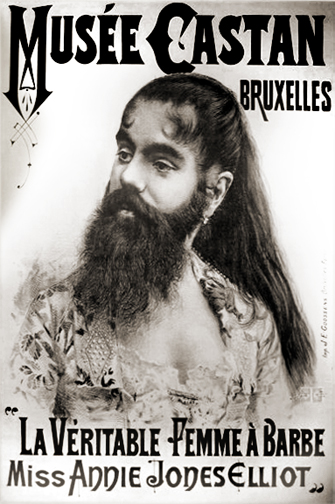
Bearded lady
A bearded lady (or bearded woman) is a woman with a naturally occurring beard normally due to the condition known as hirsutism or hypertrichosis. Hypertrichosis causes people of either sex to develop excess hair over their entire body (including the face), while hirsutism is restricted to females and only causes excessive hair growth in the nine body areas mentioned by Ferriman and Gallwey.
A relatively small number of women are able to grow enough facial hair to have a distinct beard. The condition is called hirsutism. It is usually the result of polycystic ovary syndrome which causes excess testosterone, thus (to a greater or lesser extent) results in male pattern hair growth, among other symptoms. In some cases, female beard growth is the result of a hormonal imbalance (usually androgen excess), or a rare genetic disorder known as hypertrichosis. In some cases, a woman's ability to grow a beard can be due to hereditary reasons without anything medically being wrong.
There are numerous references to bearded women throughout the centuries, and William Shakespeare also mentioned them in Macbeth:
you should be Women,
And yet your beards forbid me to interpret,
That you are so.
— 138–46; 1.3. 37–45
However, no known productions of Macbeth included bearded witches.
Charles Darwin's ideas on sexual selection that influenced the perception of women with excess facial hair were applied differently across race.[citation needed] Women of color who had excess facial hair were actually perceived as evidence of human's evolution from apes, whereas white women with excess facial hair were perceived as diseased. A beard on a white woman challenged her sex and medical condition, whereas a beard on a woman of color challenged her species.
Some famous bearded women were Krao Farini and Julia Pastrana.
Hub AI
Bearded lady AI simulator
(@Bearded lady_simulator)
Bearded lady
A bearded lady (or bearded woman) is a woman with a naturally occurring beard normally due to the condition known as hirsutism or hypertrichosis. Hypertrichosis causes people of either sex to develop excess hair over their entire body (including the face), while hirsutism is restricted to females and only causes excessive hair growth in the nine body areas mentioned by Ferriman and Gallwey.
A relatively small number of women are able to grow enough facial hair to have a distinct beard. The condition is called hirsutism. It is usually the result of polycystic ovary syndrome which causes excess testosterone, thus (to a greater or lesser extent) results in male pattern hair growth, among other symptoms. In some cases, female beard growth is the result of a hormonal imbalance (usually androgen excess), or a rare genetic disorder known as hypertrichosis. In some cases, a woman's ability to grow a beard can be due to hereditary reasons without anything medically being wrong.
There are numerous references to bearded women throughout the centuries, and William Shakespeare also mentioned them in Macbeth:
you should be Women,
And yet your beards forbid me to interpret,
That you are so.
— 138–46; 1.3. 37–45
However, no known productions of Macbeth included bearded witches.
Charles Darwin's ideas on sexual selection that influenced the perception of women with excess facial hair were applied differently across race.[citation needed] Women of color who had excess facial hair were actually perceived as evidence of human's evolution from apes, whereas white women with excess facial hair were perceived as diseased. A beard on a white woman challenged her sex and medical condition, whereas a beard on a woman of color challenged her species.
Some famous bearded women were Krao Farini and Julia Pastrana.
Recent media